عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Basic Obstetric Ultrasound الجمعة أغسطس 02, 2024 12:22 pm
Basic Obstetric Ultrasound
Backgroun
The basic obstetric ultrasound examination provides an
accurate and safe clinical assessment of the gravid uterus throughout a woman’s pregnancy including characterizing pregnancy location, identifying the number of embryos present, and aiding in the prenatal diagnosis of fetal anomalies
In 2013, the American Institute of Ultrasound in Medicine (AIUM), in conjunction with the American College of Radiology (ACR) and the American College of Obstetricians and Gynecologists (ACOG), released updated Practice Guidelines for Performance of Obstetric Ultrasound Examinations. These guidelines describe the indications and key elements of 4 major types of obstetric ultrasounds, specifically : 1.the first trimester US
2.standard second or third trimester US
3.and limited and specialized US examinations Further details regarding specific information gathered in each type of ultrasound exam is described below Also see the article Targeted Obstetric Ultrasound.
Indications
First trimester ultrasound
The first trimester basic US is typically performed to confirm a viable intrauterine pregnancy. The exam may be performed either TA or trans-vaginally. It is ideally performed before 13 weeks and 6 days of gestation. US exam at this time aids in the clinical assessment of pelvic pain and/or vaginal bleeding & vaginal bleeding in an early pregnancy because it can diagnose an
extrauterine pregnancy abnormal pregnancy, such as a A/hydatidiform molar pregnancy, an B/anembryonic gestation or or an C/incomplete versus complete abortion. A definitive diagnosis of an intrauterine pregnancy can be
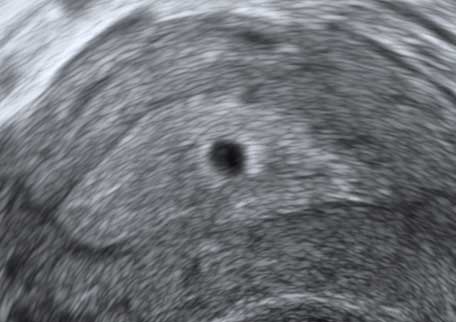
made when 1. a (GS) gestational sac containing a 2.yolk sac (YS) 3.is visualized within the uterine cavity
Without visualization of a YS or signs of a further developed pregnancy
such as an embryo, the location of the pregnancy cannot be certain
and further evaluation is warranted. In some cases where a pregnancy test is positive but there is no clear intrauterine pregnancy or extrauterine findings concerning for an ectopic pregnancy such as an adnexal mass on US, a patient may have a “pregnancy of unknown location.” It is important to consider the clinical context of a patient without a
documented intrauterine pregnancy to guide further management. This includes the patient’s 1.pelvic pain 2.vaginal bleeding 3.Serial serum beta human chorionic gonadotropin levels (bHCG),3. and pelvic exam findings. Additionally, a first trimester US is useful to diagnose an “early pregnancy loss” which is defined by American College of Obstetricians and Gynecologists as a 1. nonviable, 2. intrauterine pregnancy with 3. either an empty GS, OR a 4. GS containing an embryo or fetus without cardiac activity within the 1ST 12 & 6/7 weeks gestation. Society of Radiologists in US Multispecialty Panel on Early 1ST Trimester
diagnosis of Miscarriage and Exclusion of a Viable IUP have published conservative guidelines to aid with clinical judgment in the diagnosis of an abnormal intrauterine pregnancy. Diagnostic findings of an early pregnancy loss include: 1.) CRL of 7 mm or greater and NO heartbeat
2.) MSD of 25 mm or greater & NO embryo
3.) Absence of cardiac activity in an embryo 2 wks or more after a scan that showed a GS without a yolk sac, and/or 4.) the absence of cardiac activity in an embryo 11 days or more
after a scan that showed a GS with a YS sac.
Cardiac activity of an embryo is documented using 2-dimensional video clip or M-mode imaging If no cardiac motion is seen on TVS US in an embryo less than 7 mm,
a subsequent US in 1-2 wks is performed to assess for cardiac activity
Additionally, if patient’s clinical presentation suggests a miscarriage i.e
heavy vaginal bleeding, but she is stable for expectant management, a follow-up US performed 7-14 days after initial presentation to assess
for interval changes and viability is also appropriate management.
In the setting of a confirmed viable (IUP), the first trimester US utilized to provide an accurate gestational age (GA) assessment. IF only a GS and YS are visualized, the MSD is used to estimate GA (Mean sac diameter (mm) + 30 = gestational age in days) However, if an embryo is visualized, then a (CRL) of the fetus should be used to determine an estimated due date because it is the most accurate measurement for establishing GA
embryo should be seen by TVS US with a MGSDof 25 mm or greater. The CRL is the maximum length of the infant from cranium to caudal rump in a longitudinal plane.
Measurements of the CRL are more accurate the earlier the first trimester US is performed. If the CRL measurement is greater than or equal to 84 mm which corresponds to a GA of 14 & 0/7 wks, 2nd trimester biometric biometric parameters should be used for calculating the GA
عدل سابقا من قبل د.كمال سيد في السبت أغسطس 17, 2024 12:50 pm عدل 2 مرات
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Obsterics US الجمعة أغسطس 02, 2024 8:04 pm
In 2014, ACOG published a standardized approach for calculating a patient’s anticipated due date using both US estimates and menstrual history, specifically the patient’s first day of the last menstrual period.If the patient is unsure of her last menstrual period (LMP) or has a history of irregular menstrual cycles, dating should be calculated based on US measurements. In general, US dating is used when the discrepancy b/w menstrual dating and US dating is greater than the precision of ultrasonography. First trimester calculations are more precise compared to later gestational ages. Before 14 0/7 weeks gestation, the mean CRL calculated has a precision (accuracy) of 5-7 days.
Therefore, before 9 0/7 weeks gestation, the estimated due date should correspond to US measurements when there is more than a 5 day discrepancy between menstrual dating and US dating.
Similarly, if the US dating between 9 0/7 weeks gestation and 13 6/7 weeks gestation has more than a 7 day discrepancy from the menstrual dating, US measurements should be used to assign estimated due date. In the second and third trimester, larger discrepancies reflect less precise measurements based on biometric parameters . In the setting of multifetal gestations, amnionicity and chorionicity should be documented. In the setting of desired genetic testing, nuchal translucency measurement aids in the screening assessment for fetal aneuploidy in conjunction with biomarkers. A first trimester US is also useful for the evaluation of maternal anatomy including assessment of the uterus, cervix and adnexal structures. The presence of adnexal masses, ovarian cysts, and/or leiomyomas should be documented and followed throughout pregnancy.
Second and third trimester ultrasound
Second or third trimester US examinations use fetal biometry to assess fetal growth and also can provide detailed information on fetal anatomy. A standard obstetric US exam also may include an evaluation of : 1. fetal presentation(s)
2. amniotic fluid volume
3. cardiac activity
and placentation .4.
After the first trimester, fetal biometry specifically measures the : fetus’ biparietal diameter .1
2. head circumferences
3. abdominal circumference or average abdominal diameter 4. and femoral diaphysis length
Fetal biometry may be utilized to establish an estimated due date for a pregnancy if no prior US measurement of the embryo was done. However the most accurate gestational age assessment is based on crown rump length measurement and the variability of gestational age estimations increases throughout pregnancy. For this reason, the earliest available US should always be used to assign an estimated due date and any significant discrepancies between gestational age and fetal measurements on subsequent ultrasounds should raise suspicion for growth abnormalities. The approximate error in fetal weight prediction methods is approximately 15% and is influenced by patient body habitus, weight range of fetus, technical factors such as machine quality and experience of ultrasonographer. In the third trimester, the femur length is the best single biometric measurement of gestational age.
Assessment of fetal anomalies, also known as a fetal anatomic survey, should be performed after 18 weeks gestational age and ideally performed between 18-20 weeks gestational age.
Although it may be possible to document anatomic structures before this time, the size, position, and movement of a fetus may limit a comprehensive examination of structures and therefore require repeat US examinations.
Additionally if a fetal anomaly is detected in this preferred gestational age window (18-20 weeks), termination of pregnancy may still be an option for the patient. The basic fetal anatomic examination includes assessment of the following structures: lateral cerebral ventricles .1
2. choroid plexus 3. midline falx 4. cavum septi pellucidi 5. cerebellum 6. cistern magna 7. upper lip 8. four-chamber view of heart 9. as well as left and right ventricular outflow tracts 10. size and location of stomach 11. urinary bladder and ureters 12. spinal anatomy 13. extremities 14. and gender . A more detailed anatomic survey may be indicated depending on the risk and concern for aneuploidy. The placenta should also be further characterized at this time, specifically noting its : location .1
and proximity to the internal cervical os .2 3. as well as the number of vessels 4. and insertion site of the umbilical cord
Additionally, the second and third trimester basic US may also be used to diagnose or to monitor maternal anatomical problems, most notably cervical length in the setting of risk factors for preterm birth or cervical insufficiency. US monitoring of fibroids and/or ovarian cysts is also important, but this is limited at later gestational ages due to the size of the gravid uterus. https://emedicine.medscape.com/article/2047305-overview#a3
عدل سابقا من قبل د.كمال سيد في السبت أغسطس 03, 2024 5:34 pm عدل 1 مرات
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Basic Obstetric Ultrasound السبت أغسطس 03, 2024 12:45 pm
Limited and specialized ultrasound exam
A limited or specialized US may be performed at any gestational age and is typically used to evaluate a specific clinical concern during prenatal care. Some examples include assessment of cardiac activity when fetal heart tones are undetectable with external fetal monitoring devices to rule out fetal demise, notation of fetal presentation in setting of anticipated external cephalic version or to determine mode of delivery, and calculation of estimated fetal weight and amniotic fluid in setting of comorbidities that may predispose infants to growth abnormalities eg: chronic hypertension, pre-eclampsia, diabetes, multifetal gestation. Fetal growth evaluations are typically performed at 3-4 week intervals and usually include an assessment of amniotic fluid as well.
There are two main techniques to measure amniotic fluid in the second or third trimester, specifically single deepest pocket (SDP) OR the amniotic fluid index (AFI). The SDP technique records the 1. single 2.largest 3.vertical pocket of amniotic fluid 4.without evidence of umbilical cord or fetalparts visualized in utero. The AFI technique is the 1.summative measurement of the 2.single deepest vertical pocket of fluid without 3.evidence of cord or fetal parts noted 4.in all four quadrants of the uterus. Oligohydramnios1.(or significantly low amniotic fluid), is defined as an 2.AFI less than 5 cm OR a 3.maximum vertical pocket less than 2 cm. Polyhydramnios describes an abnormally large amount of fluid, is defined by: an 1.AFI greater than 24 cm OR a 2.single deepest vertical pocket (SDP) greater than 8 cm.
#In multifetal gestations, fluid evaluation should be performed using the SDP technique. Comparison of measurement techniques show that measurement of the SDP leads to fewer interventions (such as induction of labor for oligohydramnios) with no increase in poor perinatal outcomes.
Similar to a limited US exam, a detailedUS exam is a supplemental tool to aid in the management of prenatal care in the setting of concern for 1.fetal well-being due patient history 2.genetic screening abnormalities, or results of prior US exams. For example, The CDC and ACOG recommend that pregnant women who live in or have traveled to areas with ongoing Zika virus exposure should undergo Zika virus serologic testing and fetal ultrasonography to screen for microcephaly or intracranial calcifications as early as 3-4 weeks after symptoms or exposure. However, the CDC warned that fetal ultrasounds might not detect abnormalities until late second or early third trimester of pregnancy.
Other examples of specialized US exams include fetal surveillance with a biophysical profile, fetal Doppler US for assessment of placental insufficiency, and a more detailed anatomy scan or fetal echocardiography in setting of concern for fetal anomaly.
Safety
The prenatal US exam has been proven safe to both mothers and fetuses. As with any clinical test or medical intervention, a risk to benefit analysis of the test should be considered and should only be performed when there is a medical/obstetric indication or clinical concern. Additionally, if a diagnostic US is required for patient care it should be done under the “as low as reasonably achievable principle” (ALARA principle) due to possible risks associated to the physical effects from the exam including mechanical vibrations or increase in temperature under exam conditions as well as unknown risks of US energy to fetus not yet documented in the literature. Some ultrasonographic modalities, such as Doppler, deliver more energy to the area of interest and the use of those modalities should be reserved for specific clinical questions and an attempt made to limit their duration of use. https://emedicine.medscape.com/article/2047305-overview#a3
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Basic Obstetric Ultrasound السبت أغسطس 03, 2024 1:34 pm
Technical Considerations
Obstetric US examination requires real-time two-dimensional imaging via a trans-abdominal or trans-vaginal approach in order to adequately assess pregnancy viability through cardiac activity and fetal movement. There is currently no clinical evidence suggesting a clear advantage of three-dimensional imaging in prenatal diagnosis.
The US TXR frequency must be selected to balance optimal beam penetration versus resolution, and therefore may vary based on a patient’s body habitus. For example, a lower-frequency TXR is beneficial in obese patients to allow for increased penetration and better imaging. Modern equipment typically includes a trans-abdominal transducer with 3 to 5 MHz frequency and a trans-vaginal transducer with 5-10 MHz frequency.
Modern US equipment has boundaries set by the manufacturer, limiting the fetal exposure to energy generated by the equipment. As with any medical equipment, adequate care and maintenance should be performed as per manufacturer recommendations. Additionally, personnel involved with the use of US equipment should have appropriate training. Some US suites have quality assurance programs to evaluate performance of personnel and the US unit. The AIUM has published specific training guidelines for physicians who perform and interpret obstetric US which includes the following minimum requirements to demonstrate a strong knowledge base, technical skill and competency.Specifically for graduates of residency or fellowship programs to gain proficiency, the physician must perform at least 300 diagnostic ultrasounds. Additionally, a minimum of 170 annual diagnostic obstetric US exam is recommended to maintain the technical skills required for competency.
Procedure planning
Minimal preparation is required for a trans-abdominal or trans-vaginal US. A fasting state is not required, in contrast to other US studies (eg, GB ultrasonography). Some practitioners advise their patients to arrive to the US suite (compartment/wing) with a full bladder, but there is no consensus regarding this recommendation, especially for an obstetric US performed after 18 weeks’ gestation. If a trans-vaginal approach is to be used, the patient is asked to void just before the study to empty her bladder. This minimizes discomfort and collapses bladder for better visualization of pelvic organs. US transducers require proper cleaning before and after each patient’s use to avoid risk of microbial transmission leading to infection. Transabdominal US transducers are typically cleansed with disposable antiseptic wipes and the clean transducer may be applied directly to the patient’s skin. Conversely, trans-vaginal US transducers require more extensive cleaning and sterilization. Specifically trans-vaginal transducers should be covered with a single-use disposal cover during the patient exam. After the exam is completed, cleaning steps include1. removal of the disposal cover, 2. cleansing with running water or a damp cloth to remove residual gel or debris from probe, 3. followed by high-level disinfection chemical agents in accordance with FDA recommended guidelines. Periprocedural Care
Patient Education & Consent
Elements of informed consent
Most practitioners obtain verbal consent from patients. Ideally, this process should be initiated by the practitioner who requests the study. The *Risks, *benefits, *expectations, and *limitations of the study should be presented. Some of the limitations relate to the *inability of an US to detect all fetal anomalies, *as well as the impossibility to rule out the risk of false-negative US results. Additional consent is requested for transvaginal studies.
Equipment
The physics and principles involving US are complex, and the curious reader is encouraged to refer to other references for an in-depth discussion of those. The most important part of the US machine is the transducer, the tool that makes contact with the patient’s skin. It is equipped with piezoelectric crystals that can 1. generate a sound pulse when excited by an electric current. That sound is 2. released at a specific frequency, 3. travels through human tissue, .and 4. interacts with it based on physical properties of the tissue. Sound is 5. absorbed by the tissue, and 6. reflected back to the transducer, where the piezoelectric crystals 7. change that messageto electrical impulses that are 8. sent to the processor for interpretation. The 9. processing unit interprets the signals and creates the image we see on the screen.
Patient Preparation
For all diagnostic US studies and most, if not all, US-assisted procedures (eg, amniocentesis), anesthesia is not required.
Positioning
For abdominal studies, the patient is in a 1. supine position for most of the study, with the 2. abdomen uncovered to provide skin contact with the US TXR. She 3. may keep their clothes on. A 4. coupling gel is used b/w the TXR and the skin to reduce acoustic impedance from environmental air
This gel may be warmed for patient comfort. For transvaginal studies, the patient is to 1. remove clothing from the lower part of her body and to 2. lie in a dorsal lithotomy position. Regular stirrups may be used to assist with positioning, or the patient may be asked to assume a frog-leg position. The 3. pelvic area is covered by a blanket for the patient’s comfort. The transvaginal probe is 1. covered with a coupling gel, and 2. a vinyl or latex cover is then placed around the transvaginal US probe. 3. Another layer of gel is applied around the covered probe to *assist in the vaginal insertion and to *reduce the acoustic impedance. Some patients may feel that they are more “in control” of a transvaginal examination if they insert the vaginal probe themselves. Personnel involved in performing transvaginal studies need to be sensitive to patient’s requests. Technique
Approach Considerations
An abdominal approach is acceptable for most first- and second-trimester US examinations. In some cases, such as those involving 1. maternal obesity,2. abdominal scars due to prior surgeries,3. close evaluation of the cervical length during the second trimester, or 4. gestation less than 8 weeks, a transvaginal or translabial approach may be used. The US probe used with this approach is smaller to gain access through the vagina. In addition, the sound frequency that the probe emits is higher, as the target is closer to the probe. In general, nuchal translucency evaluation during the first trimester may be accomplished with the transabdominal approach. https://emedicine.medscape.com/article/2047305-technique
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: First-Trimester US السبت أغسطس 03, 2024 7:35 pm
Technique contd
First-Trimester Ultrasound
Approach to a first-trimester ultrasound
The first-trimester US exam is used mainly to confirm: 1. intrauterine pregnancy (IUP), 2. to confirm dating an to 3. assess nuchal translucency. The uterus, cervix, and adnexa should be evaluated for 1. location of a GS. 2. If a GS is seen, the presence or absence of yolk sac should be reported. Discriminatorylevels of human chorionic gonadotropin (hCG) and US findings have been reported. Those are quantitative levels of the pregnancy hormone beta–human chorionic gonadotropin (b-hCG) and expected US findings in a viable pregnancy. They may help predict the viability of Intrauterine Pregnancies with Uncertain Viability (IPUV). Table 1. Mean Gestational Sac Sizes at Which a Yolk Sac and an Embryo Should Be Visible
Yolk sac should be visible By TVS: WhenMSD is 8 mm (BUT 20 mmByTAS) &whenb-hCG is 7200 mIU/mLwhenGA is 5-6 wks Embryoshould be visible ByTVS : When MSD is 16 mm (BUT25 mm ByTAS) &whenb-hCG is 10.000mIU/mL whenGA is
more than 6 wks The YS can usually be visualized if the GS is approximately 1 cm in diameter. In some cases of embryonic demise, the yolk sac is deflated or irregular. Fetal*number, *location,*presence & *heart rate should be clearly evaluated and documented. An attempt to determine chorionicity should start during the first-trimester ultrasound. Thick interfaces b/w gestational sacs suggest dichorionic pregnancies, & thin or absent membranes likely represent monochorionic twins. A corpus luteumcyst (CLC) may be observed in the maternal adnexa, usually 3 cm or less in diameter. Both adnexa should be evaluated for the presence of largeovarian cysts such as occurs in ovarian hyperstimulation syndrome, & solid masses such as in ovarian neoplasm. The uterus should also be evaluated for *homogeneity, *presence, *size & *location of fibroids, especially intracavitary.
Embryonic demise
The first-trimester US presents an opportunity to identify some problematic pregnancies. Early signs of nonviable pregnancies include a *GS with an irregular shape or one that is *not growing or *b-hCG levels not correlating with ultrasonographic findings. Embryonic demise may be diagnosed when the *CRL is 6 mm without fetal cardiac activity. A study found that current guidelines regarding ultrasonographic diagnosis of
miscarriage may still be associated with misdiagnoses and should be updated to take into account gestational age.
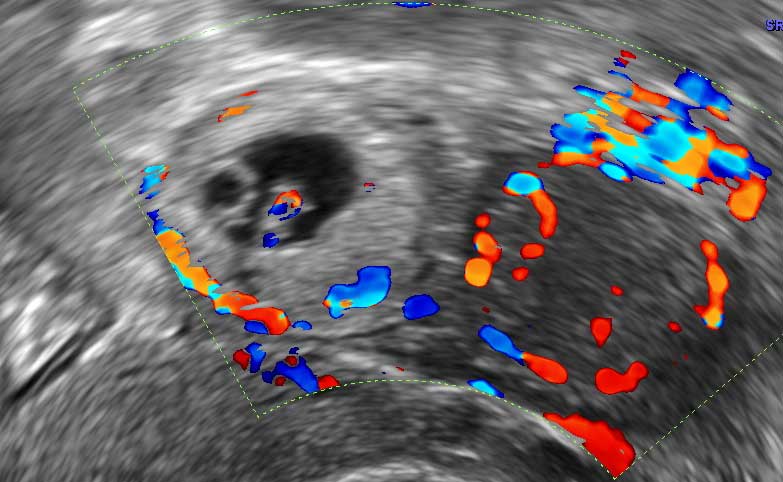
Ectopic pregnancy
Ectopic pregnancies or {Heterotopic} pregnancies, describe (one fetus inside the uterine cavity while another fetus is implanted outside the uterine cavity) may also be diagnosed. Clinically, ectopic pregnancy may manifest as 1. pelvic pain and/or 2. vaginal bleeding, 3. elevated b-hCG levels 4. free fluid in the peritoneal cavity usually representing blood, and adnexal findings.
Anencephalia
Severe fetal anomalies can also be diagnosed in the first trimester. Anencephalic fetuses present with an absent cranium on this early ultrasound examination.
First-trimester sonographic markers for aneuploidy
Aneuploidy is the presence of an abnormal number of chromosomes in a cell, for example a human cell having 45 or 47 chromosomes instead of the usual 46. It does not include a difference of one or more complete sets of chromosomes. A cell with any number of complete chromosome sets is called a euploid cell.
(AN-yoo-PLOY-dee) Is the occurrence of one or more extra or missing chromosomes in a cell or organism. Aneuploidy refers to any chromosome number that is not an exact multiple of the haploid number of chromosomes (which is 23 in humans). Early tests for aneuploidy include the 1. measurement of the skin swelling behind the fetal neck the (nuchal translucency), along with two biochemical markers :
2. pregnancy-associated plasma protein A (PAPP-A) and
3. free-hCG.
Other 4.anatomical markers for aneuploidy on the first-trimester US include :
*the absence of nasal bone
*increased frontomaxillary angle measurement based on GA
*the appearance of an objective decrease in blood flow during an atrial contraction. on ductus venosus Doppler evaluation (a-wave abnormalities)
* increased tricuspid valve regurgitation.
* a-wave abnormalities However, not all of these markers can currently be assessed in the general population.
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Obsterics US الأحد أغسطس 04, 2024 7:13 pm
Technique contd
Second- and Third-Trimester US Evaluation
Approach
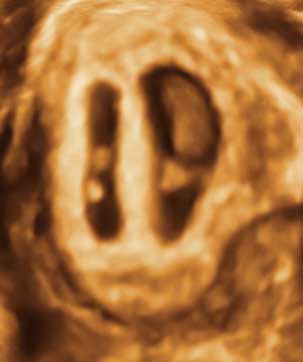
The most common indication for a second-trimester US examination is evaluation of fetal anatomy, usually b/w 18 and 20 weeks’ gestation. At this point, 1. the embryologic period is well passed, and 2. fetal organs are, for the most part, easily visualized and evaluated. The embryologic period describes the 1ST 8weeks of fetal development, (wk 3 to which are characterized by the growth and differentiation of tissues into organs . This process is known as organogenesis and occurs from weeks 3 through 8, (embryonic period). Fetal *position, *early pregnancy, *anterior placenta, *multiple pregnancies, *uterine fibroids,
and *maternal obesity, may impede a good anatomical evaluation of the fetus at this stage . If the exam is inconclusive because of one of these factors, the patient may be asked to return to finalize the fetal anatomical evaluation at a later date. Embryo at 12 weeks' gestation.
In some cases, owing to choice or lack of early access to prenatal care, patients are unable to obtain an early US examination to confirm the *gestational age (GA) of the pregnancy, *number of fetuses, and *chorionicity, which can be determined with a second-trimester ultrasound. While a first-trimester US is considered a better tool for gestational dating, the second-trimester US can be used to determine GA. A composite of multiple fetal measures is made and averaged. The common practice is not to override dates based on the calculation of last menstrual period unless there is a difference of 5 days between dates determined by last menstrual period and first-trimester US or a difference of 10 days between the last menstrual period and second-trimester US.
Multiple pregnancies
Evaluation of fetal chorionicity when multiples are present, may be performed similarly as on the first-trimester ultrasound. If the fetuses are located in 1.different gestational sacs and the 2.membrane dividing the fetuses is *thick and has a *broad base, the pregnancy is more likely dichorionic. Conversely, if the membrane dividing the twins is *thin *without a broad base, called a *(twin peak) or {delta sign}, or *absent it suggests a monochorionic pregnancy. If the fetuses are *different sexes, *dichorionic pregnancy is diagnosed.
Placental evaluation
If the patient presents with acute vaginal bleeding, ultrasound may help determine cause. Placenta previa occurs when part or the entire placenta covers the internal cervical os. This diagnosis is important, as it requires cesarean delivery.
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Basic Obstetric US الإثنين أغسطس 05, 2024 12:44 pm
Technique contd Fetal ultrasound testing Fetal well-being may be evaluated with various measures. A biophysical profile (BPP) is composed of a series of measurements to assess fetal hypoxia. They include : 1.amniotic fluid evaluation 2.breathing movement 3.gross body movements, and 4.fine movement. A scoring system consisting of either 0 or 2 points is then applied to the fetal evaluation. Measurement of the fetal umbilical artery (UA) Doppler, indicateis the resistance that fetal blood flow finds at the placental level. To obtain fetal UA Doppler, the angle of insonation should be as close to zero degrees to the umbilical artery as possible. A comparison of forward blood flow b/w fetal systole and diastole is obtained. A large systolic-to-diastolic ratio indicates higher resistance of blood flow at the placental level. Maternal anatomy to be evaluated includes the *uterus, *adnexa and *cervix
Fetal structures to be evaluated include the *head *face *neck *cerebellum *choroid plexus cisterna*magna *lateral cerebral ventricles *midline falx *cavum septi pellucidi & *upper lip. Most of the fetal syndromes, aneuploidies, and severe fetal anomalies manifest as fetal CNS anomalies. A normal US finding does not completely rule out fetal aneuploidies but is reassuring. If the patient had a prior pregnancy complicated by CNS anomalies, the risk of recurrence in a later pregnancy is about 2%.
Fetal growth
Similarly, by following the same parameters measured to obtain GA on the second-trimester US, the pregnancy may be monitored for objective estimation of fetal growth. Clinically, fetal growth is monitored by measuring the fundal height during routine obstetric visits. Fetal measurements obtained to determine fetal ageand weight include :*biparietal diameter head *circumference *abdominal circumference *femur length *humerus length. When growth of fundal height is not as expected in some twin pregnancies or others pregnancies at risk for growth restriction, serial second- and third-trimester ultrasounds may be performed to evaluate adequate fetal growth. Because of variability in US measurements, a 3-week wait between growth ultrasounds is used to determine fetal growth. Fetal head circumference should be measured in a plane that includes the cavum septum pellucidum, falx cerebri, and thalamus. To measure the biparietal diameter (BPD), the calipers should be placed from the outside of the calvarium proximally to the inside of the calvarium distally, crossing the falx cerebri at a 90° angle. The same anatomical landmarks used to measure the biparietal diameter are used to measure the fetal head circumference. This measurement is obtained by measuring the outer circumference formed by the calvarium. Head measurements may be helpful to indicate *fetal age, *microcephaly, or *macrocephaly. Objectively, the cephalic index (CI) is defined as the width of the head divided by the length in a percentage scale. The normal value is b/w 70 and 80, but an abnormal value does not necessarily indicate pathology. If the cephalic index is more than 80, the fetal head will have a rounded appearance, also called brachycephalia & may be seen in trisomy 18. If the cephalic index is less than 70, the head may appear flat, also known as dolichocephalia & may be seen is preterm babies or craniosynostosis. Minor changes in the shape of the fetal head are normal. https://emedicine.medscape.com/article/2047305-technique?icd=login_success_email_match_norm#c3
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Basic Obstetric Ultrasound الإثنين أغسطس 05, 2024 7:01 pm
Technique contd
Fetal anatomy: CNS
The cerebellum is located in the posterior inferior aspect of the brain. It has a large mass of cerebral cortex above and the Pons below. It is divided in two hemispheres. The cerebellar surface folds into itself, increasing the area. Those folds are called lobules. There are 3 major areas: the *flocculonodular, *anterior, and *posterior lobes. This organ has more neurons than the rest of the brain. The functions are related to *gait, *language, and *body tone. Fetal evaluation of the cerebellum includes its *presence *shape and *size. During a second-trimester US, cerebellum is measured by the outer length of the posterior cerebellar hemispheres, at the same plane that the septum cavum pellucidum, cisterna magna, and nuchal fold are seen. Posterior fossa deformities are seen with Chiari II malformations (also called Arnold-Chiari), in which parts of the cerebellum and brainstem are pulled downward into the foramen (ovale ???? magnum) owing to a spinal defect. The sonogram shows obliteration of the posterior fossa structures, usually with elongation of the cisterna magna (banana sign) and flattening of the frontal cephalic bones (lemon sign). The cisterna magna is also located in the posterior fossa, posterior to the cerebellum. It is part of the openings of the subarachnoid space. Dilatation of the cisterna magna may occur in conditions such as Dandy-Walker malformation, in which there is an abnormal *communication b/w the fourth ventricle and the cisterna magna *via a defect in the cerebellar vermis. The human brain has 4 choroid plexus. They are built as a *filter b/w the *blood and the cerebrospinal fluid *(CSF) and consist of *many blood vessels separated from the ventricular space by *choroid epithelial cells that, by *passive and active transport, *maintain the balance of the cerebrospinal fluid. They are located in the *superior horn of the lateral ventricles. On US, they appear as a *bright half-moon–shaped echo area in the ventricle. *Choroid plexus cysts are found in 1 per 100 fetuses with trisomy 18; however, if the only abnormal finding is a choroid plexus cyst, the risk for trisomy 18 is 1 in 477. The American College of Obstetricians and Gynecologists (ACOG) recommends considering amniocentesis if there are other “soft” markers for aneuploidy, if the blood markers for aneuploidy are abnormal, or if the mother will be aged 32 years at the time of term delivery. A choroid plexus that is *floating in the lateral ventricle is called a floating or “drooping” choroid,
which is *caused by an enlarged lateral ventricle The ventricular system of the brain is composed of the *lateral ventricles, the*third and the *fourth ventricles. Cerebrospinal fluid (CSF) is produced by *blood *filtered by *ependymal cells on the *choroid plexus. CSF travels along all ventricles to be reabsorbed through the arachnoid villi
During second-trimester US, the lateral ventricles are measured in a plane where the cavum septum pellucidum is visible anteriorly, from the internal membranes of the lateral ventricles just behind the choroid plexus. A blockage from the reabsorption system may cause an enlarged lateral ventricle, with increased CSF pressure, which is called ventriculomegaly, a condition seen with hydrocephalus. If the cause of the hydrocephalus is not evident, it is called simple hydrocephalus. In some cases, hydrocephalus may occur along with other conditions such as Dandy-Walker malformation or agenesis of the corpus callosum. The cavum septum pellucidum (CSP) is composed of *two different layers of grayand white matter. The*space b/w the two layers is the cavum, which *disappears during adult life. It is *closely related to the corpus callosum.*Absence of the cavum on a second-trimester US may indicate absence of the corpus callosum, which may be *associated with multiple syndromes, including *trisomy 13 or *18 or Dandy-*Walker malformation. Agenesis of the corpus callosum may be confirmed with ultrasound of the midcoronal planes.
Fetal anatomy: SPINE:
The spinal evaluation of the fetus begins with an anatomic assessment of the head, abnormalities of which reflect some spinal problems. For instance, Chiari II malformations are often seen in fetuses with spina bifida. Owing to the decreased pressure in the spine, contents of the posterior fossa herniate through the foramen magnum into the spinal canal. There is displacement of the cerebellar vermis, fourth ventricle, and medulla oblongata. The cistern magna enlarges, becoming banana-shaped. The frontal bones collapse and the head may take on a lemon shape. The most common spinal anomalies are the ones associated with spina bifida, in which failure of the vertebral bones to close allows part of the spinal cord to lie outside the neural canal. In cases of spina bifida occulta, the vertebral schisis (split/cleft) is covered with skin, and it may appear as a lipoma or dimple at birth. If the defect is open, it is referred as a spina bifida aperta, and it is further classified as a meningocele if it is covered by a thin meningeal membrane or myelomeningocele (if the sac contains neural tissue). The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) recommends that, when possible, a longitudinal section of the fetal spine should be obtained to screen for open and closed spinal dysraphism (spina bifida). Targeted fetal neurosonography is recommended if there is suspicion of a brain or spinal abnormality during the obstetric ultrasound examination.
Fetal anatomy: Chest
The fetal chest evaluation includes the fetal heart and lungs. The chest view should include a 4-chamber heart and outflow tracts, if possible. A detailed cardiac US is beyond the scope of this article and is reserved for patients with a prior history
of a fetus with *cardiac anomalies, patients with *overt diabetes, suspicions of a *syndrome that affects the fetal heart, and patients with *abnormally appearing fetal cardiac anatomy based on second-trimester ultrasound. In the evaluation of the fetal heart, the position of the fetal heart in relation to the fetal body should be assessed first. The fetal stomach and the apex of the fetal heart should be on the left side of the fetus. Next, a 4-chamber view of the fetal heart should be obtained. The transverse view of the fetal heart is obtained right above the fetal diaphragm. With minor adjustments, a 4-chamber view is acquired. The apex should be pointing to the left side, and the right ventricle should be the most anterior chamber. The upper chambers should be equal in size to the lower chambers, and both sides should be of similar size during both systole and diastole. This view allows the sonographer to evaluate the interventricular septum. The size of the heart should be about half the size of the whole thorax.
Movement evaluation during this view includes free movement of both atrioventricular valves, as well as the foramen ovale flap in the left atrium. In some cases, an echogenic intracardiac focus that represents calcifications on the papillary muscle is seen and is a marker for fetal aneuploidy. With this view, more than half of the congenital cardiac anomalies may be detected, including those related to cardiac position, cardiac septa, cardiac chambers, and masses. Left outflow and right outflow views may be obtained, if possible. Additional cardiac views may be obtained for a more complete fetal cardiac evaluation. These include the long axis of the left ventricle, short axis of the great vessels, aortic arch, and pulmonary artery view. Fetal heart tones may be visible as early as 5 weeks’ gestation. The 5 components of the fetal heart motion to be evaluated include rate, rhythm, atrioventricular association, structural anomalies, and evaluation for hydrops. The fetal heart rate may change during the course of the pregnancy but should generally be between 110 and 180 beats per minute. Routinely, an M-mode picture of the fetal heart is taken. Fetal heart rhythm may be constant or variable; minor variability is normal, but significant rate variability should be noted, and, if the fetus is viable, the obstetrician should be notified immediately.
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Basic Obstetric Ultrasound الثلاثاء أغسطس 06, 2024 12:55 pm
Technique contd
Fetal anatomy:diaphragm
The fetal diaphragm is evaluated for continuity. Congenital diaphragmatic hernia is the most common anomaly in the fetal thorax if cardiac problems are excluded. They are difficult to observe with US tend to grow as the pregnancy progresses. The diagnosis may be made upon observation of *loops of bowel in the thorax or *discontinuity of the diaphragm muscle. Cysts in the region of the lungs may result from cystic adenomatous hyperplasia or bronchopulmonary sequestration. There is hamartomatous involvement in cystic adenomatous hyperplasia, and the prognosis depends on the size and type. In bronchopulmonary sequestration, a portion of the bronchopulmonary system develops separately and is seen as a hyperechoic area at the lung base.
Fetal anatomy: Abdomen
Components of the abdominal-area evaluation should include : *presence *size *position and of *the stomach *kidneys *bladder *umbilical cord insertion site into the fetal abdomen *and umbilical cord vessels. The plane for abdominal circumference should include : the outer margins of a transverse plane that includes the fetal *stomach,*spine *liver and the *umbilical portion of the left portal vein equidistant from both sides of the abdomen. A small circumference may indicate a growth-restricted fetus. The fetal liver can be evaluated *for size and presence of *masses or *cysts. Liver calcifications have been described as part of fetal viral infections. A “double-bubble” stomach indicates duodenal atresia, a marker for Down syndrome. Absence of the fetal stomach may be related to other fetal anomalies. Esophageal atresia may be diagnosed with 1.US based on the absence of a visible fetal stomach and the presence of 2.polyhydramnios; however, the diagnostic yield with US is only about 50%. Bowel dilatation may indicate 1.large-bowel obstruction or 2.anal atresia. Hyperechoic bowel is seen in cases of 1.meconium, 2.bleeding or 3.cystic fibrosis. Two anterior abdominal defects are worth mentioning : 1.Omphalocele is a *midline defect *covered by a *membrane. If the defect is large enough, it may include the fetal liver. *The association with fetal syndromes is high. 2.Gastroschisis is *a lateral defect to the umbilical cord, *NOT covered by a membrane. On *US, it is visualized as free loops of bowelin the amniotic sac. It has been *associated with some fetal syndromes, but at a lower rate than omphalocele. Fetal kidneys are located *on both sides of the fetal spine, with an *ovoid shape in a longitudinal view and a round shape in a transverse view. Fetal kidneys *enlarge with GA; therefore, they are easier to visualize as pregnancy progresses and the fetus grows. It is not routinely necessary to measure the kidneys. Care should be *taken in NOT confuse the fetal adrenal gland as part of the kidneys, as it may be larger than in adults.*Minor fluid collection in the kidneys is normal, BUT more than 4 mm before 32 weeks’ gestation OR more than 7 mm after 32 weeks’ gestation fluid collection (pyelectasis) may be a marker of aneuploidy. In fetuses who present with obstruction of the renal outlet, the affected kidney is visualized on US *as a paraspinal sac *cysts or *abnormal ureteral dilatations. Absence of kidneys is rarer but carries a lethal prognosis. Polycystic kidneys are a *bilateral disorder *representing tubular ectasia, usually *appearing after the second trimester. Meckel-Gruber syndrome is characterized by 1.polycystic kidneys with 2.encephalocele and 3.polydactyly. Fetal bladder is 1.seen as a hypoechoic area 2.caudally on the fetus. The 2.filling cycle of the bladder is 60-90minutes; therefore if an initial view of the fetus does not demonstrate a bladder, repeat imaging is recommended. In rare cases such as in urinary obstruction, the identification of fetal sex is medically indicated. The umbilical cord may be evaluated by applying color Doppler interrogation to the area around the bladder and visualizing the two umbilical arteries around the bladder. Care should be taken to obtain a transverse view of the fetal abdomen and not to confuse the fetal iliac arteries.
Fetal anatomy: Extremities
The *presence or *absence of fetal extremities should also be documented. This is done *by demonstrating one bone in the proximal extremity and two bones distally. Measurement of *the long bones is obtained to evaluate fetal growth. A single-center study by Dicke et al indicated that although US exam allows most cases of abnormal hand position, limb reduction defect, and arthrogryposis to be detected prenatally, at least 20-25% of these abnormalities will probably be missed. Arthrogryposis describes congenital joint contracture in two or more areas of the body. It derives its name from Greek, literally meaning 'curving of joints'. The sensitivity of US was found to be as follows: Polydactyly: 19.1% Abnormal hand position: 76.0% Limb reduction defect involving the long bones: 76.1% Arthrogryposis: 81.3% https://emedicine.medscape.com/article/2047305-technique?icd=login_success_email_match_norm&icd=login_success_email_match_norm#c3
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Normal labor الثلاثاء أغسطس 06, 2024 8:31 pm
Normal labor Labor is the process through which a fetus and placenta are delivered from the uterus through the vagina. Labor is a process that subdivides into three stages. The first stagestarts when 1.labor pains begin and ends2.with full cervical dilation (10 cm) 3.and effacement. The second stagecommences with 1.complete cervical dilation and ends with 2.the delivery of the fetus. The third stageinitiates 1.after the fetus is delivered and ends when the 2.placenta is delivered. This activity outlines the stages of labor and its relevance to the interprofessional team in managing women in labor. Effacement means, the cervix stretches and gets thinner. Dilation means that the cervix opens. As labor nears, the cervix may start to thin (efface) and open (dilate). This prepares the cervix for the baby to pass through the birth canal (vagina). Successful labor involves three factors: 1.maternal efforts and uterine contractions2.fetal characteristics, and 3.pelvic anatomy. This triad is classically referred to as the passenger, power, and passage Serial 1/cervical examinations are used to determine *cervical dilation, *effacement, and fetal *position. And 2.Fetal heart monitoring is employed nearly continuously to assess fetal *well-being throughout labor. Also 3.Cardiotocography is used to monitor the *frequency and *adequacy of contractions. Medical professionals use the information they obtain from monitoring and cervical exams to determine the patient's stage of labor and monitor labor progression. Initial Evaluation and Presentation of Labor Women will often self-present to obstetrical triage with concern for the onset of labor. Common chief complaints include 1.painful contractions 2.vaginal bleeding/bloody show 3.and fluid leakage from the vagina. It is up to the clinician to determine if the patient is in labor, defined as 1.regular, 2.clinically significant contractions with an 3.objective change in cervical dilation and/or effacement. When women first present to the labor and delivery unit, 1/vital signs are obtaied & reviewed for any abnormalities, including *temperature *heart rate *oxygen saturation *respiratory rate and *blood pressure. The patient should be placed on 2/continuous cardiotocographic monitoring to ensure fetal wellbeing. The 3/patient's prenatal record, including 1.obstetric history 2.surgical history 3.medical history 4.laboratory, and 5.imaging data, should undergo review. Finally, a 4/Record of present illness 1.review of systems 2.physical exam, including a 3.sterile speculum exam During which, clinicians will look for signs of rupture of membranes such as
amniotic fluid pooling in the posterior vaginal canal. To insure that a rupture of membranes has occurred, additional testing such as *pH testing, *microscopic exam looking for ferning of the fluid, or *laboratory testing of the fluid can be the next step. Amniotic fluid has a pH of 7.0 to 7.5, which is more basic than normal vaginal pH. The fern test is based on the ability of amniotic fluid to form a microscopic crystalline pattern that resembles fern leaves when the fluid air dries on a glass slide. Performed by authorized providers in the point of care. A 5/sterile gloved exam should be done to determine the degree of cervical dilation and effacement. The measurement of cervical dilation is made by *locating the external cervical os and *spreading one's fingers in a ‘V’ shape, and estimating the *distance in centimeters between the two fingers. It is approximately 10 cm when CX is fully dilated
Then 6/Effacement is measured by *estimating the percentage remaining of the length of the thinned cervix compared to the *uneffaced cervix. Then 7/During the *cervical exam, confirmation of the presenting fetal part is necessary. *Bedside US can be employed to confirm the presentation and position of the fetal presenting part. Particular mention should be noted in the case of *breech presentation due to its increased risks regarding fetal *morbidity and *mortality compared with the cephalic presenting fetus. Management of Normal Labor Labor is a natural process, but it can suffer interruption by complicating factors, which at times necessitate clinical intervention. The management of low-risk labor is a delicate balance between allowing the natural process to proceed while limiting any potential complications. During labor, cardiotocographic monitoring is often employed to monitor uterine *contractions and fetal *heart rate over time. Clinicians monitor fetal heart tracings to evaluate for any signs of *fetal distress that would warrant intervention as well as the *adequacy or inadequacy of contractions. Vital signs of the mother are taken at regular intervals and whenever concerns arise regarding a clinical status change. Laboratory testing includes the *hemoglobin *hematocrit & *platelet count and is sometimes *repeated following delivery if significant blood loss occurs. Cervical exams are usually performed *every 2 to 3 hours unless concerns arise and warrant more frequent exams. Frequent cervical exams are associated with a *higher risk of infection, especially if a rupture of membranes has occurred. Women should be allowed to ambulated freely and change positions if desired.
An intravenous catheter is typically inserted in case it is necessary to *administer medications or fluids. Oral *intake should not be withheld. If the patient remains without food or drink for a prolonged period of time, intravenous fluids should be considered to help replace losses but do not need to be used on all laboring patients. Analgesia is offered in the form of 1.intravenous opioids 2.inhaled nitrous oxide and 3.neuraxial analgesia in those who are appropriate candidates. Amniotomy is considered on an as-needed basis for fetal *scalp monitoring or *labor augmentation, but its routine use should be discouraged. Oxytocin may be initiated to augment contractions If found to be inadequate. https://www.ncbi.nlm.nih.gov/books/NBK544290/
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Normal labor الأربعاء أغسطس 07, 2024 1:12 pm
First Stage of Labor The first stage of laborbeginswhen true labor pains starts and ends with full cervical dilation to 10 centimeters.
Labor often begins*spontaneously or may be *induced medically for a variety of maternal or fetal indications. Methods of inducing labor include : 1.cervical ripening with prostaglandins 2.membrane stripping, 3amniotomy & 4.intravenous oxytocin. Although precisely determining when labor starts may be inexact, labor is generally defined as beginning when contractions become : 1.strong and 2.regularly spaced at approximately 3 to 5 minutes apart.
Women may experience painful contractions throughout pregnancy that do not lead to cervical dilation or effacement, referred to as false labor. Thus, defining the onset of labor often relies on retrospective or subjective data.
The first stage of labor is further subdivides into two phases, defined by the degree of cervical dilation. The latent phase is commonly defined as the 0 to 6 cm, while the active phase commences from 6 cm to full cervical dilation. The presenting fetal part also begins the process of engagement into the pelvis during the first stage. Throughout the first stage, serial cervical exams are done to determine the *position of the fetus *cervical dilation and *cervical effacement. Cervical effacement refers to the cervical length in the anterior-posterior plane. When the cervix is completely* thinned out, and *no length is left, this is referred to as 100 percent effacement. The station of the fetus is defined relative to its position in the maternal pelvis. When 1.the *bony fetal presenting part is *aligned with the maternal ischial spine, the fetus *is 0 station. when 2.Proximal to the ischial spines are stations -1 centimeter to -5 centimeters, and 3.distal to the ischial spines is +1 to +5 station.
During the latent phase of 1ST stage of labor, the 1.cervix dilates slowly to approximately 6 centimeters. The latent phase is generally considerably 2.longer and 3.less predictable with regard to the rate of cervical change than is observed in the active phase. A normal latent phase can 4.last up to 20 hours and 14 hours in nulliparous and multiparous women, respectively, without being considered prolonged. Sedation can 5.increase the duration of the latent phase of labor.
The cervix 1.changes more rapidly and predictably in the active phase until it 2.reaches 10 centimeters and 3.cervical dilation and effacement are complete. 4.Active labor with more rapid cervical dilation generally starts around 6 centimeters of dilation. 5.During the active phase, the cervix typically dilates at a rate of 1.2 to 1.5 centimeters per hour. Multiparas, or women with a history of prior vaginal delivery, tend to demonstrate more rapid cervical dilation. The absence of *cervical change for *greater than 4 hours in the *presence of adequate contractions or six hours with inadequate contractions is considered the arrest of labor and may warrant clinical intervention.
https://www.ncbi.nlm.nih.gov/books/NBK544290/
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Normal labor الأربعاء أغسطس 07, 2024 1:59 pm
Second Stage of Labor The second stage of labor1/commences withcomplete cervical dilation to 10 centimeters and ends
with the delivery of the neonate. This was also defined as the pelvic division phase by Friedman. After 2/cervical dilation is complete, the fetus 1.descends into the vaginal canal with or without maternal pushing efforts. The 2.fetus passes through the birth canal via 7 movements known as the cardinal movements : A/engagement B/descent C/flexion D/internal rotation E/extension F/external rotation and G/expulsion.
In women who have delivered vaginally previously, whose bodies have acclimated to delivering a fetus, the second stage may only require a brief trial, whereas a longer duration may be required for a nulliparous female. In parturients (giving birth) 3/without neuraxial anesthesia, the second stage of labor typically lasts less than three hours in nulliparous women and less than two hours in multiparous women. In women 4/who receive neuraxial anesthesia, the second stage of labor typically lasts less than four hours in nulliparous women and less than three hours in multiparous women.
If the second stage of labor lasts longer than these parameters, then the second stage is considered prolonged. Several elements may influence the duration of the second stage of labor, including fetal factors such as fetal *size and position, or maternal factors such as *pelvis shape, the *magnitude of expulsive efforts *comorbidities such as hypertension or diabetes *age, and history of *previous deliveries. https://www.ncbi.nlm.nih.gov/books/NBK544290/
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Normal labor الخميس أغسطس 08, 2024 12:18 pm
Third Stage of Labor The third stage of labor commences when the 1.fetus is delivered and concludes with the 2.delivery of the placenta. Separation of the placenta from the uterine interface is hallmarked by three cardinal signs, including : a 1.gush of blood at the vagina 2.lengthening of the umbilical cord & a 3.globular shaped uterine fundus on palpation. Spontaneous expulsion of the placenta typically takes between 5 to 30 minutes. A delivery time of greater than 30 minutes (Retained Placenta), is associated with a higher risk of : post 1.partum hemorrhage and may be an indication for 2.manual removal or other 3.intervention. Management of the third stage of labor involves 1.placing traction on the umbilical cord with 2.simultaneous fundal pressure to effect faster placental delivery. The function of the stages of labor is to create a universal definition that medical professionals can use to communicate with each other about labor. The stages of labor can be used to help determine where the patient is on the labor spectrum. Clarifying the stages of labor has helped create guidelines, which define normal and abnormal trends in labor. Clinical management also gears toward the various stages of labor. Complications may arise during any of the stages of labor to result in abnormal labor. During the first stage, women may experience the arrest of parturition, necessitating cesarian delivery, which may carry greater maternal or fetal risk. Second stage complications include a variety of complications related to the trauma of the delivery process to either the fetus or the mother. The fetus can suffer 1.acidemia 2.shoulder dystocia 3.bony fractures, nerve 4.palsies, scalp 5.hematomas and 6.anoxic brain injuries
Similarly, the mother can develop a host of traumatic complications ranging from 1.uterine rupture, vaginal 2.laceration 3.cervical laceration 4.uterine hemorrhage 5.amniotic fluid embolism, and 6.death. The third stage of labor may encounter complications from hemorrhage, 1.cord avulsion 2.retained placenta, or 3.incomplete removal of the placenta.
Clinical Significance of the stages of labor
Defining the stages of labor with a specific beginning and end has allowed clinicians to study labor trends and to create labor curves. For example, in the 1950s, Dr. Friedman created a graphical representation of the rate of normal labor during latent and active labor using observed clinical data. These, in turn, can be used to determine if a woman is progressing through labor as expected and helping to identify abnormal labor. Friedman observed that labor typically has a sigmoidal shape when measured by cervical dilation over time. During the active phase of labor, cervical dilation occurs at a rate of 1 centimeter or more per hour. If dilation occurs much slower, the patient may be at risk for abnormal labor or arrest of labor.
If a woman is found not progressing through the first stage of labor as expected, this could lead to the diagnosis of the arrest of dilation or descent, which could result in cesarean delivery. The findings of Dr. Friedman have recently been challenged, and the current consensus is the normal latent phase of labor lasts longer than was previously observed. The criteria for the stages of labor create a universal language that allows healthcare professionals to communicate with one another about patient care accurately. Also, specific interventions are tailored to particular stages of labor to try to create better patient outcomes. For example, active management in the third stage of labor is carried out by placing immediate traction on the umbilical cord and administering intravenous oxytocin, which correlates with a lower risk of postpartum hemorrhage. Clinicians will continue to use the stages of labor to guide labor management and study labor patterns to improve patient care.
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Basic Obstetric US Steps الخميس أغسطس 08, 2024 6:06 pm
US allows accurate estimation of 1.GA 2.determination of fetal viability
3.fetal presentation position 4.of the placenta 5.measurement of Amniotic fluid 6.estimation of fetal wt identification of 7.multiple pregnancies 8.identification of some fetal abnormalities Preparing for the scan * explain the process & the indications for the scan to the pt * make sure she is ready to proceed & if she has any questions * scan is performed with pt lying supine to the RT of yu & facing yu * pt is properly coverd & her clothing protected from US gel * Apply the gel over her lower abdomen * Select the suitable probe & preset for the GA & BMI of the pt * Hold the probe with yur RT hand & operate the machine controls with yur LT hand * Placing the probe in transverse position on the lower abdomen, using
the marker as a reference to make sure that the RT side of the pt is
displayed on the LT side of the screen, yu can check this by placing yur finger beside the probe on the abdomen. * place the probe in longitudinal position, & using the marker as a
reference that the uterine fundus should be displayed on the LT side of the screen, & the maternal UB on the RT * To keep the image orientation correct, rotate probe in a clockwise
direction when changing from a transverse plane to longitudinal plane, and Anticlokwise when changing from longitudinal to transverse
* Always keep the orientation of the probe consistent, & don't rotate more than a 100 degrees The probe can only be moved in FOUR ways: 1.Sliding i.e moving probe while touching the skin, from side to side & up & down 2. Rotating i.e clockwise & anticlockwise 3. Dipping i.e heel-toe 4. Angling i.e anteriorly (forwards) & posteriorly (backwards) The standerdized 6-step approach of how to examine & measure the fetus Step 1 : Determination of fetal Presentation & Position 1/Begin by placing probe on the center of the lower abdomen just above the symphysis in transverse position 2/ Angle probe forwards & backwards to identify the presenting fetal part Step 2 :
Detection of fetal heart beat Maintaining a transverse orientation, Slide (move) the probe UP towards the Umbilicus
to identify the fetal heart beat Step 3 : Identification of number of fetuses in the uterus Maintaining the transverse orientation, slide the probe up the RT side of the uterus from the /1. symphysis to the fundus 2/ Repeat this sliding movement on the center of the uterus 3/ Also repeat on the LT side of the uterus * The size of the uterus will determine whether 2 or 3 sweeps are 4/ required To complete this step, Rotate the probe to a longitudinal position, & survey the whole uterus by sliding the probe from
the RT side to the LT above & below the umbilicus 5/ Keep the probe perpendicular to the floor as yu slide Step 4 : Determination of location & position of the placenta 1/ Maintaining a longitudinal orientation starting at the RT fundus, slide the probe down towards the symphysis, keeping it perpendicular to the floor
2/ Slide along the three previous Tracks - RT lower abd up to RT fundus, center of uterus, LT lower abd to LT fundus 3/ Slide the probe into the midline & using small movements, locate the leading edge of the placenta in relation to the internal os Step 5 : Estimation of Amniotic Fluid 1/ Mentally, divide the maternal abdomen & the uterus into Four quadrants 2/ Keeping the probe in longitudinal orientation& perpendicular to the floor, slide it from the lower RT quadrant through the other Three quadrants 3/ Identify the deepest vertical pocket of the amniotic fluid in each, that does not contain fetal parts or umbilical cord. 4/ Measure by placing the calipers at 90 degrees to the horizontal. 5/ The Amniotic Fluid Index (AFI) Is the sum of these Four measurements * The deepest vertical pocket (DVP) IS the largest measurement of the four * Be ware here of reverberation artifact that can make yu under estimate one or more of these measurements Step 6 : Fetal Biometric Measurements 1/ to take biometric measurements, apply the 1st sweep & planes for 5,7,11of easy walk standardized 20 planes
2/ Perform the 1ST sweep by rotating the probe to obtain a longitudinal section of the fetus 3/ Identify the positions of the fetal head & long axis of its body 4/ The 1ST measurement to take is the Biparietal Diameter (BPD) and Head Circumference (HC)
* From the longitudinal axis of the fetus, rotate the probe at 90 degrees the level of the fetal head * Angle, Rotate, & then Dip the probe to obtain the correct head shape
and the Intracranial Land marks which indicate the trans-ventricular plane known as (plane 4) * Take the BPD at the widest point across the skull. The BPD can be measured from outer TO outer, OR outer TO inner * To obtain an outer to outer BPD measurement, place the calipers on the outer edge of both upper & lower parietal bones * To obtain an outer to inner BPD measurement, place the Lower caliper on the inner border of the Lower parietal bone 5/ Next, measure the Head Circumference (HC) by placing the Ellipse caliper on the outer parietal bone. * Then rotate from the trans-ventricular plane to the trans-cerebellar plane (plane 6) by keeping the Cavum Septum Pellucidum in view & rotating the probe towards the fetal neck 6/ Measure the trans-cerebellar diameter (TCD) by placing the linear caliper across the maximum diameter of the cerebellum 7/ Rotate back to the trans-ventricular plane & slide the probe down through the fetal chest & yu will observe the heart beating, this is (plane 7) (just at the level LT to the umbilicus) 8/ To measure the abdominal Cirumference (AC) yu may need to make small movements of angling & rotatation of the probe. This will allow yu to maintain a transverse orientation of the fetus * Plane 11 is where a landmark visible of a stomach & a small central portion of the umbilical vein * Place the Elipse caliper on the outer edge of the fetal abdomen
and measure the AC 9/ The final stage of the scan is to measure the femur length (FL) * Maintaining a transverse section of the fetal body slide the probe down from plane 11 towards the fetal pelvis - at upper maternal abdomen- AND rotate it to view a longitudinal section of the femur * This technique will prevent from accidentally measuring the humerus * Place the calipers at each end of the femur & measure the longest visible diaphysis. Be sure to measure along the long axis of the femur
* Don't include spur artifacts on the end of the diaphysis
Scanning procedure is now complete Aftercare of the pt 1. Clean the probe & return it safely on the holder on the US sacanner 2. Clean pt abdomen & allow her to sit up 3. Now wash yur hands 4. Check the measurements on the screen 5. Explain the scan report to the pt, & get her the apportunity to ask any questions 6. Provide her with a handwritten report to pass it to her care givver
7. She is now free to leave
8. Provide pt with a written report 9. Prepare yur machine for the next scan
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: OBS short notes الأربعاء أغسطس 14, 2024 7:33 pm
Meaning of Obstetrics Relating to the care and treatment of women in childbirth and during the period before and after delivery. OR relating to childbirth or obstetrics what is obst Ultrasound
Obstetric US, also known as prenatal or pregnancy US, uses high-frequency sound waves to produce images of a developing embryo or fetus. The procedure also monitors the health of the mother's uterus, ovaries, and the blood flow through the umbilical cord to the placenta. the best time for a single US examination The American College of Obstetricians and Gynecologists (2016), recommended that without other specific indications, the best time for a singleUS examination is between 18 and 22 weeks' gestation. Preparing for TAS A full UB is very important for the US exam.
1.Empty UB 90 minutes before exam time 2. then consume one 8-ounce glasses of fluid: water, milk, coffee, etc~ an hour before exam time
3. We recommend a two-piece outfit so as to access pt abdomen without you removing clothing. Determing gender
1. The accuracy of determining baby's gender increases with GA .
2.The accuracy varies from 70.3% at 11 weeks to 98.7% at 12 weeks, and 100% at 13 weeks 3. Eleven weeks is the earliest that sex determination can be carried out with an US using a method called the 'nub theory'.Jul 17, 2023 4. The ideal time for a gender reveal US is during the second trimester, typically B/W 18 and 22 wks of pregnancy. OBS vs pelvic US
Obstetric/pregnancy US, routinely used to assess the growth and health of unborn babies during pregnancy.
female pelvis US, used to look at the female pelvis, uterus, cervix, fallopian tubes and ovaries, with a TVS or Trans-abdominal transducer. Baby sex organs development The internal sex organs – the testes in boys and the uterus and ovaries in girls – look the same until9 wks of pregnancy. The external sex organs – the penis in boys, the clitoris and labia majora in girls – don't start to differ from each other until about 11 weeks.Jul 6, 2022 OBS sepsis score The Sepsis in OBS Score is a validated pregnancy-specific score to identify risk of ICU admission for sepsis with the threshold score of 6 having a negative predictive value of 98.6%." A score of less than 6 rules out the need for ICU admission Accuracy of OBS US The US scan isn't 100 per cent accurate, BUT the advantages of US that it's non-invasive,
painless, NON-ionizing radiation and safe for both mother and unborn baby. If fetal abnormalities are detected, you may be offered further tests to confirm the diagnosis, such as amniocentesis and chorionic villus sampling. Types of Pregnancy Scan Early pregnancy or dating scan (8-11 weeks) Nuchal Translucency scan (11-14 weeks) Early Anomaly scan (14-18 weeks) Fetal Anomaly scan (19-23 weeks) Growth scan or Fetal Wellbeing scan (24-42 weeks) Recommended at 36 weeks. Optional - four weekly, more frequently in some conditions.
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: OBS short notes الخميس أغسطس 15, 2024 1:02 pm
What is an ultrasound?
Ultrasound (also calledsonography or ultrasonography) is a noninvasive imaging test. An US picture is called a sonogram. Ultrasound uses high-frequency sound waves to create real-time pictures or video of internal organs or other soft tissues, such as blood vessels. Ultrasound enables healthcare providers to “see” details of soft tissues inside your body without making any incisions (cuts). And unlike X-rays, ultrasound doesn’t use radiation. Although most people associate ultrasound with pregnancy, healthcare providers use ultrasound for many different situations and to look at several different parts of the inside of your body.
How does an ultrasound work?
During an ultrasound, a healthcare provider passes a device called a transducer or probe over an area of your body or inside a body opening. The provider applies a thin layer of gel to your skin so that the ultrasound waves are transmitted from the transducer through the gel and into your body. The probe converts electrical current into high-frequency sound waves and sends the waves into your body’s tissue. You can’t hear the sound waves. Sound waves bounce off structures inside your body and back to the probe, which converts the waves into electrical signals. A computer then converts the pattern of electrical signals into real-time images or videos, which are displayed on a computer screen nearby.
What are the different kinds of ultrasounds?
There are three main categories of ultrasound imaging, including: Pregnancy ultrasound (prenatal ultrasound). Diagnostic ultrasound. Ultrasound guidance for procedures. Pregnancy ultrasound Healthcare providers often use US (often called prenatal or obstetric US) to
monitor you and the fetus during pregnancy. Providers use prenatal US to: Confirm that you’re pregnant. Check to see if you’re pregnant with more than one fetus. Estimate how long you’ve been pregnant and the gestational age of the fetus. Check the fetal growth and position. See the fetal movement and heart rate. Check for congenital conditions (birth defects) in the fetal brain, spinal cord,
heart or other parts of its body. Check the amount of amniotic fluid. Most healthcare providers recommend an US at 20 weeks pregnant. This test
tracks the fetus’s growth and development during pregnancy. This US may also
show the biological sex of the fetus. Tell your technician if you do or do not want
to know the sex. Your provider may order extra scans to get answers to any questions or concerns,
such as the potential for congenital conditions. Diagnostic ultrasound Providers use diagnostic US to view internal parts of your body to see if something
is wrong or not working properly. They can help your provider learn more about
what’s causing a wide range of symptoms, such as unexplained pain, masses (lumps)
or what may be causing an abnormal blood test. For most diagnostic US exams, the technician places the TXR on your skin.
In some cases, they may need to place the probe inside your body, such as in
your vagina or rectum. The type of diagnostic ultrasound you have, depends on the details of your case. Examples of diagnostic ultrasounds include: Abdominal US: An US probe moves across the skin of your midsection (belly) area. Abdominal ultrasound can diagnose many causes of abdominal pain. Kidney (renal) US: Providers use kidney ultrasound to assess the size, location and shape of your kidneys and related structures, such as your ureters and bladder.
Ultrasound can detect cysts, tumors, obstructions or infections within or around your kidneys. Breast US: A breast US is a noninvasive test to identify breast lumps and cysts.
Your provider may recommend an ultrasound after an abnormal mammogram. Doppler US: a special US technique that assesses the movement of materials,
like blood, in your body. It allows your provider to see and evaluate blood flow
through arteries and veins in your body. Doppler US is often used as part of a
diagnostic ultrasound study or as part of a vascular ultrasound. Pelvic US: A pelvic US looks at the organs in your pelvic area between your lower abdomen (belly) and legs. Some of the pelvic organs include your bladder, prostate, rectum, ovaries, uterus and vagina. Transvaginal US: Your provider inserts a probe into your vaginal canal.
It shows reproductive tissues such as your uterus or ovaries.
A transvaginal US is sometimes called a pelvic US because it evaluates structures
inside your pelvis (hip bones). Thyroid US: Providers use ultrasound to assess your thyroid, a butterfly-shaped endocrine gland in your neck. Thy can measure the size of your thyroid and see
if there are nodules or lesions within the gland. Transrectal us: provider inserts an ultrasound transducer into your rectum.
It evaluates your rectum or other nearby tissues, such as the prostate in people
assigned male at birth. Ultrasound guidance for procedures Providers sometimes use US to perform certain procedures precisely.
A common use of US is to guide needle placement to sample fluid or tissue from: Tendons. Joints. Muscles. Cysts or fluid collections. Soft-tissue masses. Organs (liver, kidney or prostate). Transplant organs (liver, kidney or pancreas). Examples of other procedures that may require ultrasound guidance include: Embryo transfer for in vitro fertilization. Nerve blocks. Confirming the placement of an IUD (intrauterine device) after insertion. Lesion localization procedures.
What is the difference between a 3D ultrasound and a 4D ultrasound?
For US during pregnancy, the traditional US is a two-dimensional (2D) image of the fetus. 2D US produces outlines and flat-looking images, which allows your health provider to see the fetus's internal organs and structures. Three-dimensional (3D) US allows the visualization of some facial features of the fetus and
possibly other body parts such as fingers and toes. Four-dimensional (4D) US is 3D ultrasound in motion. Providers rarely use 3D or 4D fetal US
imaging for medical purposes, though it can be useful in diagnosing a facial or skeletal issue. They do, however, use 3D US for other medical purposes, such as evaluating uterine polyps and fibroids. While US is generally considered to be safe with very low risks, the risks may increase with unnecessary prolonged exposure to US energy or when untrained users operate an US machine. Because of this, the U.S. Food and Drug Administration (FDA) advises against getting a 3D US for non-medical reasons such as for “keepsake” moments or entertainment.
Who performs an ultrasound?
A doctor or a healthcare provider called an US technician or sonographer performs USs. They’re specially trained to operate an ultrasound machine properly and safely. It’s important to always have your US performed by a medical professional and in a medical facility.
Test Details
How do I prepare for an ultrasound?
The preparations will depend on the type of US you’re having. Some types of ultrasounds require no preparation at all. For US of the pelvis, including US during pregnancy, of the female reproductive system and of the urinary system, you may need to fill up your bladder by drinking water before the test. For Abdominal US, you may need to adjust your diet or fast (not eat or drink anything except water) for several hours before your test. In any case, your healthcare provider will let you know if you need to do anything special to prepare for your ultrasound. They may give you instructions during an appointment or when scheduling your ultrasound. Instructions may also be available in your electronic medical records if you use such a system.
What happens during an ultrasound?
Preparation for an US varies depending on what body part to be scanned. Your provider may ask you to remove certain pieces of clothes or change into a hospital gown. Ultrasounds that involve applying the transducer (probe) over your skin (not in your body)
follow these general steps: You’ll lie on your side or back on a comfortable table. The US technician will apply a small amount of water-soluble gel on your skin over the area to be examined. This gel doesn’t harm your skin or stain your clothes. The technician will move a handheld transducer over the gel to get images inside your body. The technician may ask you to be very still or to hold your breath for a few seconds to create clearer pictures. Once the technician has gotten enough images, they’ll wipe off any remaining gel on your skin and you’ll be done. An US test usually takes 30 minutes to an hour. If you have any questions about your specific type of ultrasound, ask your healthcare provider.
Is an ultrasound painful?
USs that are performed externally (over your skin) are generally not painful. You won’t feel the sound waves that US uses. If asked to have a full bladder for the procedure, it may be uncomfortable. It may also be uncomfortable to lay on the exam table if you’re pregnant. Ultrasounds that go inside body cavities, such as your vagina or rectum, may be uncomfortable, but they shouldn’t hurt.
Are ultrasounds safe?
Yes, research to date has largely shown US technology to be safe with no harmful side effects. US doesn’t use radiation, unlike some other medical imaging tests, such as X-rays and CT scans. Still, all US should be done by a professional who has training in using this specialized technology safely.
Results and Follow-Up
When should I know the results of my ultrasound?
The time it takes to get your results depends on the type of ultrasound you get. In some cases, such as prenatal US, your provider may analyze the images and provide results during the test. In other cases, a radiologist, a healthcare provider trained to supervise and interpret radiology exams, will analyze the images and then send the report to the provider who requested the exam. Your provider will then share the results with you or they may be available in your electronic medical record (if you have an account set up) before your provider reviews the results.
What conditions can be detected by ultrasound?
Ultrasound can help providers diagnose a wide range of medical issues, including: Abnormal growths, such as tumors or cancer. Blood clots. Enlarged spleen. Ectopic pregnancy (when a fertilized egg implants outside of your uterus). Gallstones. Aortic aneurysm. Kidney or bladder stones. Cholecystitis (gallbladder inflammation). Varicocele (enlarged veins in the testicles). What questions should I ask my healthcare provider about my ultrasound? If you need an ultrasound, you may want to ask your provider the following questions: What type of ultrasound do I need? What should I do to prepare for my ultrasound? Do I need any other tests? When should I expect to get test results? A note Ultrasounds are common, safe and effective imaging tests. Make sure you get an ultrasound from a well-trained professional (sonographer) who understands how to use this technology properly. If you have any questions about your specific ultrasound test, talk to your healthcare provider. They’re available to help. https://my.clevelandclinic.org/health/diagnostics/4995-ultrasound
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Early Pregnancy Complications الخميس أغسطس 15, 2024 6:12 pm
Early Pregnancy Complications The main reason for early pregnancy scans is to confirm that the pregnancy is developing normally and to rule out miscarriage. Miscarriage is the most common of early pregnancy complications which affects approximately one in every six early pregnancies. However, not all women who experience pain and bleeding suffer miscarriage and US scans are necessary to see if pregnancy is developing normally despite women having symptoms. Other early pregnancy complications include ectopic pregnancy, when a pregnancy grows outside the cavity of the uterus. Ectopic pregnancies are relatively rare compared to miscarriage, but they are potentially more harmful to women’s health and it is important to diagnose them as soon as possible. US can also be used to determine how old pregnancy is if a woman is not certain of her last period or has irregular cycles. The accuracy of ultrasound in dating early pregnancy is +/- five days.
How early can a healthy pregnancy be seen on ultrasound scan?
The earliest an US scan can identify a healthy intrauterine pregnancy is 17 days after the egg was released from the ovary(ovulation). This is approximately three days after a missed period. Pregnancy tests are more sensitive and they become positive a few days before the period is missed, so there is a window of about a weekb/w the earliest positive urine pregnancy test and the earliest the pregnancy becomes visible on scan. Normal early pregnancy four days after missed period
How does early pregnancy look on ultrasound scan?
For the first two weeks after a missed period, early pregnancy appears on the scan as a small fluid filled bubble as the embryo (future baby) is too small to be seen yet. The embryo with heartbeat is first seen 12-17 days after the missed period (i.e. at around six weeks’ gestation calculated from the first day of the last menstrual period). The presence of the heartbeat is a very reassuring sign, which indicates that the risk of pregnancy miscarrying is low. From then on, the embryo grows very quickly and three weeks after a missed period head and body can be seen on the scan. Four weeks after the missed period many fine details of the embryo can be seen including brain, spine, arms and legs. The heart rate also increases rapidly and peaks at four to five weeks after the missed period (8-9 weeks’ gestation).
When is the best time to attend for an early pregnancy scan?
1.Women who have positive urine pregnancy test and who experience vaginal bleeding or lower abdominal pain should attend for early pregnancy scan without delay regardless how many weeks they are pregnant
2.Women who are well but had a miscarriage in their previous pregnancy should attend for the scan three weeks after the missed period (at seven weeks’ gestation) when the embryo and heartbeat can be clearly seen. Women who had previous ectopic pregnancy should attend for the scan one to two weeks after the missed period (five to six weeks’ gestation) to check for the location of pregnancy.
Live embryo three weeks after missed period
Miscarriage
Miscarriage is diagnosed on US when there is a fetal pole (an embryo) visible, but the NO heart beat.
When a miscarriage happens very early in pregnancy before the embryo develops, the diagnosis of
miscarriage is not always straightforward and sometimes repeated scans are needed before the diagnosis
could be reached.
In many cases of miscarriage, the pregnancy is passed naturally (spontaneous) from the uterus by strong contractions and with bleeding. US may be helpful to determine whether the natural process of miscarriage
has been completed or whether surgery or medical intervention may be required to speed recovery.
Ectopic pregnancy (EP)
Early pregnancy complications which are located outside the uterine cavity are described as ectopic
pregnancies. They are relatively rare and they occur in 1-2% of all pregnancies.
The most common location of ectopic pregnancy is in the Fallopian tube, but they may occur
anywhere in the pelvis.
Risk factors for tubal ectopic pregnancy are 1.history of pelvic infection 2.history of infertility 3.and
increased maternal age. Women who fall pregnant 4.whilst using coil for contraception and those
who have had an 5.ectopic pregnancy in the past , are at particularly high risk of having an EP.
US is the only method which provides a reliable diagnosis of ectopic pregnancy prior to surgery.
All our consultants are experts in the ultrasound diagnosis of ectopic pregnancy.
In some cases, an EP may lead to serious internal bleeding and prompt, accurate diagnosis helps to
avoid delays in referring women for emergency surgery.
The majority of women with ectopic pregnancies present with mild symptoms, which do not require immediate operation. In these cases, US helps to identify those women in whom EP is likely to resolve
naturally without causing harm.
Our consultants have been in the forefront of research in the management of EP for many years and have developed a diagnostic approach which helps more than a third of women with ectopic pregnancies to
overcome the condition without needing surgery or medical treatment.
Tubal ectopic pregnancy
Caesarean scar pregnancy
This type of EP occurs when a pregnancy implants into a hole in the uterine muscle caused by poor healing
after previous Caesarean section.
Women who had two or more Caesarean sections are at particularly high risk of developing these early pregnancy complications.
The diagnosis of Caesarean scar pregnancy is not always easy and it requires a high level of US skill.
The main risk of Caesarean scar pregnancy is severe bleeding from the uterus which can happen even
when pregnancy is very early and can lead to a hysterectomy and loss of woman’s fertility.
We also have particular interest in the diagnosis and management of Caesarean scar pregnancy and
other rare ectopic pregnancies such asA/cervical, B/interstitial and C/intramural pregnancy.
Our team is particularly well known for their expertise in the diagnosis and management of Caesarean
scar ectopic pregnancy and we regularly see women with this condition who are referred to us from all
parts of the UK and many European countries.
Live Caesarean scar pregnancy
Pregnancy of unknown location (PUL)
Sometimes pregnancy cannot be seen on the scan although the urine pregnancy test is positive. This is described as a pregnancy of unknown location (PUL). In most cases this is because miscarriage had happened before women attend for the scan. It usually takes for a couple of weeks for pregnancy hormones to clear after miscarriage which explains why the pregnancy test is still positive. Some women are not sure when they may have fallen pregnant and they may attend for the scan before pregnancy is large enough to show on ultrasound. A small proportion women with PUL are diagnosed with ectopic pregnancy on follow up scans. We have developed our own highly effective method for assessing women presenting with PUL. We carry out a blood test to measure of hormones ß-hCG and progesterone.
When combined, the reading of hormone levels in blood helps us to determine whether a miscarriage had already occurred OR whether a pregnancy is still developing and further follow up scans are needed. This enables us to provide most women with a conclusive diagnosis on the same day and avoid unnecessary follow up visits and stress caused by prolonged diagnostic uncertainly
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: FAQs الخميس أغسطس 15, 2024 7:40 pm
FAQs Is it possible to diagnose ectopic pregnancy on the scan? Experienced operators are able to detect almost all EPs measuring more than a few millimetres in size on ultrasound scan. It is important to emphasize; however, that EPs tend to develop more slowly than intrauterine pregnancies and it often takes them longer to grow to the size which makes them visible on the scan. Most women with a positive pregnancy test in whom US cannot identify a pregnancy have either normal pregnancies which are younger than expected from the date of their last period or they have
already suffered a miscarriage. A small proportion of these women; however, may develop small ectopic pregnancies. A blood test is usually arranged in these cases to measure the levels of pregnancy hormones in women’s blood. Based on the result of the blood test we can advise pts on the likely outcome of their pregnancy and on the need for further follow up.
When can you see the baby’s heartbeat? The earliest US can confirm the presence of a heartbeat is two weeksafter a missed menstrual period ORfour weeksafter conception. In women who conceive after IVF the heartbeat can be seen four weeks after the day of oocyte collection. Again, in order to avoid coming for the scan too early it is best to delay the attendance until two and a half to three weeks after the missed period or four and a half to five weeks after conception/oocyte collection.
Conception usually occurs around 11-21 days after the first day of the last period of a woman who has a regular period. The estimation of conception date is based on this, but is rarely ever exact since it is difficult to know exactly when ovulation occurs. The earliest an USscancan identifya healthy IUPis 17 days after the egg was released from the ovary (ovulation). This is approximately three days after a missed period. When conception occures Conception occurs b/w 12 and 24 hours after ovulation. The two major factors in conception: are the timing of sexual intercourse with ovulation. Therefore, if you know the first day of period, you can add 11 to 21 days to this day to have an idea of when conception occurred. For example, if you are pregnant and your last period started on March 5, that means you likely conceivedbetween March 16 and 26.Jan 12, 2024 Is US accurate in determining conception?
Fetuses grow quickly, and they also follow the same pattern of growth in virtually every case. That means, by measuring size of the fetus and looking for certain distinguishing characteristics
an ultrasound can give an accurateestimate of when you conceived.Sep 25, 2023 t's typically not until a woman is six weeks pregnant that any part of the fetus is visible
which allows the doctor to determine whether a pregnancy will be viable. How many days delay in period confirms pregnancy?
A late period is when a cycle doesn't start as expected, in a normal cycle lasting b/w 24 to 38 days. When a period is seven days late, she may be pregnant although other things may cause a late or skipped period. What is earliest positive pregnancy test? In many cases, you might get a positive result from an at-home test as early as 10 days after conception. For a more accurate result, wait until after you've missed your period to take a test. Remember, if you take a test too soon, it could be negative even if you're pregnant. Causes of a positive pregnancy test with no pregnancy in US? The most common reasons for a pregnancy not appearing on the US scan are:
it is 1.too soonto see the baby on the scan. 2.you have had a miscarriage. the 3.pregnancy is outside the womb (an ectopic pregnancy)
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: FAQs الجمعة أغسطس 16, 2024 3:55 pm
FAQs CONTD How soon an US confirms pregnancy
Most practitioners wait until at least 6 weeks to perform the first pregnancy ultrasound. However, 1.a GS can be seen as early as 4 1/2 weeks after last period, & 2.a fetal heartbeat can be detected at 5 to 6 weeks (though that isn't always the case). When to start showing pregnancy?
Typically, your bump becomes noticeable during the second trimester. B/w16-20 weeks, your body will start showing your baby's growth. For some women, their bump may not be noticeable until the end of the second trimester and even into the third trimester. The second trimester starts in the fourth month.
Is it safe to have a scan in early pregnancy? There is no evidence that US scans can harm pregnancies. It is important to ensure, however, that the energy of US beam is kept As Low As Reasonably Achievable (ALARA "radiation principle"). Use of pulsed Doppler (PWD) devices to measure blood flow should be avoided in the first weeks of pregnancy as their energy output is higher compared to the US beam used for standard imaging. Our equipment is fully compliant with the international standards for safe use in pregnancy and the machine energy output is continuously monitored during the examination.
Can you see Fallopian tubes on the scan? Normal Fallopian tubes are very thin and they cannot be routinely seen on the scan. If the tubes are damaged, they tend to fill with fluid which makes it possible to see them. Tubal patency can be tested using a procedure called HyCoSy which is described in the section on the services we offer to women with concerns about their fertility.
Hysterocontrastsonography (HyCoSy Procedure)
A speculum is placed in the vagina (like having a smear test). A thin plastic catheter attached to a syringe is then passed through the neck of the (cervix). Water and dye is injected through the catheter. The flow of the water and dye is observed into the uterus and fallopian tubes with internal US.
What if I am allergic to Latex? Allergy to Latex is rare, but it can sometimes cause severe anaphylactic reactions. If you think that you may be allergic to Latex please let us know so that we can avoid using gloves and probe covers which contain Latex during your examination.
Is there a risk of infection? Our infection control policies are very stringent and we employ very elaborate procedures for cleaning of the US probes. Prior to and after each examination the probes are thoroughly cleansed
using antiseptic agents. The probes are then placed into a level disinfection device (Trophon) which is considered to be the best currently available method for cleaning US TXRs. Our doctors wear gloves during examinations and disposable probes covers are always used to provide additional protection from infection.
Can I have a scan if I am bleeding? Vaginal bleeding does not affect quality of ultrasound diagnosis and scans can be safely performed during menstrual periods or on those with abortion or those who are experiencing irregular vaginal bleeding.
Are ultrasound scans painful? Transvaginal US scans should not cause any significant discomfort and they are much easier to tolerate than smear tests. Transvaginal scans cannot be performed on unmarried women and in these women transabdominal scans are preferable. In menopausal pts with vaginal dryness, transvaginal examinations may be more uncomfortable. In order to minimise discomfort application of a lubrication gel containing local anaesthetic may make the examination easier to tolerate. Alternatively, local application of hormone oestrogen in the form of vaginal tablets or cream for one to two weeks prior to the examination may also be helpful.
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: symptoms & signs of pregnancy الجمعة أغسطس 16, 2024 9:02 pm
Symptoms of early pregnancy Significant hormonal changes take place during pregnancy. These
trigger a variety of symptoms. Some women experience many of the symptoms of pregnancy, while others may have only a few. Symptoms of early pregnancy include : 1.missed periods 2.breast changes 3.tiredness 4.frequent urination 5.nausea and vomiting (morning sickness). However, these symptoms may be caused by other factors and do not necessarily mean that you are pregnant, so if you suspect you are pregnant take a home pregnancy test and see your GP. A wide range of changes can occur in your body in the later stages of pregnancy, including : backache, headache, leg cramps or varicose veins, itch or tingling, constipation, haemorrhoids or indigestion, vaginitis or vaginal discharge, or mood changes or
depression. See your GP right away if you experience symptoms like vaginal bleeding or breaking waters, chronic pain, high temperature, severe headaches or vision loss. Signs of Pregnancy The signs of early pregnancy can include: 1.missed period 2. nausea and vomiting (often called ‘morning’ sickness, but it can occur at any time) 3. breast tenderness and enlargement 4. fatigue 5. passing urine more frequently than usual, particularly at night 6.cravings for some foods, distaste for foods you usually like, and a sour or metallic taste that persists even when you’re not eating (dysgeusia). Many of pregnancy signs, such as a missed period (amenorrhoea), nausea (morning sickness) or tiredness can also be caused by stress or illness, so if you think you are pregnant take a home pregnancy test (urine test) or see your GP, who will administer a urine test, blood test or ultrasound scan. Missed Period Missing a period is often the first sign of possible pregnancy. However, some women experience light bleeding around the time of their expected period.
Nausia & Vomiting
‘Morning’ sickness is a condition that affects more than half of all pregnant women. The symptoms include nausea and vomiting, and loss of appetite. Many women with morning sickness don’t just get symptoms in the morning but experience them throughout the whole day.
Morning sickness usually begins around the fourth to sixth week of pregnancy and may settle by week 12, although it can continue for longer or return at around 32 weeks.
Breast changes
During pregnancy, the breasts become fuller, swollen and tender. These changes are similar to those you may have noticed in the few days before your period During pregnancy, theskin around the nipplebecomes darker and the
veins in the breast become more obvious.
Fatigue
Overwhelming tiredness is common in early pregnancy. 1/This is most likely caused by the 1.massive increase in the sex hormone progesterone. Progesterone is A/needed to maintain the pregnancy and help the B/baby to grow, but it C/also slows your metabolism. Try to get some more sleep or rest when you can during this early stage. Your 2/energy levels will probably rise again by around the fourth month of pregnancy when the placenta is well established. Tiredness during pregnancy can also be 2.caused by anaemia, which is most commonly caused by iron deficiency. Eating iron-rich foods is important to prevent iron deficiency anaemia during pregnancy. Medical treatment of anaemia in pregnancy usually involves taking iron tablets & Sometimes an iron infusion is needed.
This needs a hospital admission but only takes a few hours
Some iron infusions can be given by your GP.
Frequent urination
Pregnancy causes 1.an increase in levels of body fluids and greater kidney efficiency. The increased uterus size, 2.also presses against the bladder. As a result
most pts start experiencing more frequent urination within the first few
weeks of becoming pregnant.
Food cravings
Cravings (intense desire & appetite) for certain foods are very common in pregnancy, especially for foods that provide energy and calcium, such as milk and other dairy products. You may also notice a sudden distaste for foods you previously liked. Some women even develop an unusual taste for non-food items such as soil or paper. This is called ‘pica’ and may indicate a nutrient deficiency
Please speak to your GP or midwife if this develops. Other Symptoms of Pregnancy Many of these symptoms may also be indicative of other conditions. If in doubt, see your GP. backache breathlessness constipation haemorrhoids (piles) headaches heartburn and indigestion itchy skin leg cramps mood changes (such as unexplained crying) tingling and numbness in your hands vaginal discharge vaginitis varicose veins and leg oedema (swelling)
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: symptoms & signs of pregnancy السبت أغسطس 17, 2024 2:11 pm
Backache
Back pain during pregnancy can affect more than 1 in 3 women. This is usually due to loosening of ligaments and change in posture due to the growing baby. You can help reduce back pain during pregnancy by wearing flat heeled shoes, using chairs with good back support, avoiding lifting heavy objects, and doing gentle exercise. Exercising in water can reduce back pain in pregnancy, and physiotherapy and acupuncture may also help.
Breathlessness
At the onset of pregnancy the hormone progesterone increases your lung capacity. This enables you to carry more oxygen to your baby and get rid of waste products such as the carbon dioxide that you both produce. At each breath you breathe more deeply and the amount of air you inhale (and exhale) increases significantly. This can make you feel short of breath. In addition, as pregnancy approaches term, the pressure of the enlarging uterus and baby on your diaphragm can make your breathing feel more laboured. Contact your doctor or midwife if you experience sudden onset of breathlessness associated with any of the following: pain palpitations (heart pounding) extreme tiredness exercise.
Constipation
Constipation refers to infrequent, hard bowel motions that are difficult to pass. Constipation is a common problem in pregnancy that is caused by pregnancy hormones slowing your gastrointestinal movement, or by pressure of growing uterus on your rectum. If you experience constipation during pregnancy, you are advised to: drink plenty of water every day. increase your dietary fibre (such as bran, wheat and fresh fruit and vegetables). do gentle, low impact exercise such as swimming, walking or yoga. Don't take over-the-counter laxatives without first consulting your midwife or GP. If changes to your diet and lifestyle don't make a difference, then your GP or midwife can prescribe a laxative that is safe to use in pregnancy.
Haemorrhoids (piles)
You may develop haemorrhoids (piles) as a result of straining from constipation or the pressure of your baby’s head. Be reassured, symptoms usually resolve on their own soon after birth. If you have bleeding from haemorrhoids, itching, discomfort or pain it is recommended that you : 1. Alleviate or prevent constipation by increasing your daily water and fibre intake 2. Sit in warm salty water for about 15 minutes, especially after a bowel motion 3.Apply haemorrhoid cream If the bleeding or pain continues, talk with your GP (doctor) or midwife.
Headaches
Contact your GP or midwife if you have a headache during pregnancy that is not relieved by paracetamol, such as Panadol, especially in the second half of pregnancy. A persistent headache can be associated with pre-eclampsia – a condition that can 1.affect your kidneys and thus 2.increase blood pressure and 3.decrease blood flow to your baby.
Heartburn and indigestion
Heartburn, reflux or indigestion is pain and discomfort associated with acid from the stomach entering and ‘burning’ the oesophagus. Indigestion is more common during pregnancy due to 1.the pressure of the enlarging uterus on the organs of the abdomen and 2.the action of progesterone that relaxes the muscle b/w the oesophagus and stomach(gastro-esophageal sphincter). If you are experiencing heartburn, reflux or indigestion, it is recommended that you : Eat small and more frequent meals .1 2.Avoid eating just before going to bed 3. Sleep with extra pillows so your head is raised 4. Wear loose-fitting clothing 5. Avoid any food or fluid that aggravates symptoms – such as fatty foods containing ,fried foods, fatty meats and pastry, spicy foods including curry and chilli, alcohol & caffeine including tea, coffee, chocolate and cola Consult your doctor before taking antacids. If these strategies do not relieve your symptoms, please consult your GP, who may prescribe a medication that will safely reduce the secretion of acid.
Itchy skin
Widespread itching over the body is not common in pregnancy but it can be very distressing, interfering with sleep and enjoyment of pregnancy. Dry skin and eczema are the most common causes but sometimes there may be no apparent cause for the itching. In rare cases, where the palms of the hands and soles of the feet are itchy, it may be due to serious liver disease – a blood test can be done to check for this. An itchy rashlater in pregnancy, is thought to be caused by the body’s reaction to the stretching of the skin. This is called PUPPS. Itching can be controlled using moisturisers and antihistamines. Ask your doctor or midwife what antihistamines are safe in pregnancy.
Leg cramps
Leg cramps occur due to a build-up of acids that cause involuntary contractions of the affected muscles. They are experienced by up to half of pregnant women, usually at night. Leg cramps are more likely in the second and third trimesters. If you experience leg cramps, it is recommended that during an episode you: Walk around .1 2. Stretch and massage the affected muscle(s) to disperse the build-up of acids. 3. Apply a warm pack to the affected muscle(s).
If you find cramps troublesome, discuss with your GP or midwife the option of taking magnesium lactate or citrate morning and evening.
Mood changes
Some newly pregnant women experience mood changes such as irritability. Other pregnant women experience feelings of elation. It is thought that the pregnancy hormonesinfluence chemicals in the brain, causing mood changes. During pregnancy, 1 in 10 women experience depression. Depression is treatable, so if you are feeling depressed or ‘down’ during pregnancy it is extremely important to get help early. Please contact your GP (doctor), midwife or maternal and child health nurse as soon as possible.
Tingling and numbness in your hands (carpal tunnel syndrome)
Carpal tunnel syndrome – tingling and numbness in your hands – affects up to 60 % of women during pregnancy. It is caused by compression of the median nerve due to an increase in the tissue fluids during pregnancy. Carpal tunnel syndrome may be mild, intermittently painful, or severe, which may cause partial paralysis of the thumb or loss of sensation. Symptoms usually resolve on their own soon after birth. If you are experiencing tingling and numbness in your hands, inform your doctor or midwife. In very severe cases, your doctor may recommend corticosteroid injections or surgical treatment.
Vaginal discharge
An increase in vaginal discharge is a common change during pregnancy. If it is associated with itchiness, pain, a bad odour or pain on passing urine then it may be due to an infection. Seek treatment from your GP.
Vaginitis
Vaginitis is inflammation of the vagina, and is a distressing complaint for many women. It is more frequent during pregnancy. Some causes of vaginitis include vaginal thrush, bacterial vaginosis, trichomoniasis and chlamydia. See your GP for diagnosis and treatment
Varicose veins and leg Oedema (swelling)
Varicose veins of the legs are very common in pregnancy due to a combination of factors, including 1.increased volume of circulating blood during pregnancy, and 2.pressure of the pregnant uterus on the larger veins. This 3.increased pressure on the veins can also result in swelling of the legs (oedema) that can cause : *pain *feelings of heaviness *cramps especially at night *and other unusual sensations. If you have varicose veins, it is recommended thWear support stockings. 1. Avoid standing for long periods. 2. Exercise gently and regularly (walking or swimming). 3. Lie down to rest with feet elevated, when you can. 4. Try massaging your legs. Tell your doctor or midwife at your next pregnancy visit
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Pregnancy tests السبت أغسطس 17, 2024 7:16 pm
Pregnancy tests
How do pregnancy tests work?
A pregnancy test checks your blood or urine for a hormone Human Chorionic Gonadotropin (hCG). This is a hormone made by the placenta Placenta provides growing baby with oxygen and nutrients from your bloodstream throughout the pregnancy. The amount of hCG in yur blood & urine rise steeply during the 1ST 12 wks
of pregnancy and then fall to low levels for the rest of the pregnancy
Home pregnancy test kits
Home pregnancy test kits are available from pharmacists. These kits offer accurate readings (up to 99 %) if performed strictly according
to the manufacturer’s instructions. However, many women who use home pregnancy test kits get inaccurate results. The most common mistake is to test for pregnancy too soon after the missed period. The manufacturer’s instructions will tell you when is the best time to use the kit. It is very important to follow the manufacturer’s instructions exactly.
How to use a home pregnancy test kit
Home pregnancy test kits vary in their sensitivity to hCG. Most test kits are best used about one to two weeks after last period.
most home pregnancy tests follow the same basic principles: Urine is collected in a small container, dip the test strip into the urine. Alternatively, some kits offer a test strip that you hold under your stream of urine. To improve accuracy of results, it is best to test your urine when you first get out of bed. Early morning urine is concentrated and contains higher levels of hCG than at other times of the day. Most test strips indicate the presence of hCG by the appearance of a coloured line or dot. Results are rapid. Most test kits take only a few minutes to complete. Most kits come with a second test strip. This allows you to test again at a later stage.
Positive result
If test is positive (no matter how faint the line, colour or sign is), you should see your GP doctor or family planning clinic to confirm the result with a 1.blood test OR 2.another urine test. Beware that false-positive and false-negative results can happen. False positive: Although rare, this can happen if : you have 1.blood OR 2.protein in urine. Certain3.drugs can also cause this A/tranquilisers B/anticonvulsants C/hypnotics D/fertility drugs . Other reasons for false positive results are: A 3.dirty urine collecting cup. Detergent residue, is known to cause false-positive results A 4.faulty test kit for example, A/damaged kit B/Expired date
C/exposed to heat or moisture A 5.recent birth or miscarriage, because a woman’s blood and urine may still contain detectible levels of hCG for a few weeks afterwards an 6.ovarian tumour or some other type of hCG-producing growth.
Negative result
If you get a negative result, you are probably not pregnant BUT false-negatives can happen if: you didn’t follow the instructions correctly 1. the test is out-of-date 2. you tested too soon after the pregnancy began 3. your urine was too diluted 4. you are taking certain medicines, including antihistamines. If you suspect you may be pregnant, see your doctor and ask for a blood pregnancy test to confirm the result
Always see your doctor for confirmation
If a home pregnancy test gives a negative result, yet you feel that you are pregnanT: 1. Trust your instincts 2. Treat yourself as if you are pregnant until proven otherwise. 3. Avoid cigarettes and alcohol. 4. Make an appointment with your doctor. Pregnancy tests performed in laboratories are 99 per cent accurate.
Blood pregnancy tests used by doctors
Your doctor can give you a blood pregnancy test as early as 11 to 14 days after ovulation. To perform a blood pregnancy test, the doctor draws blood from a vein in your arm. This blood is sent to a laboratory for testing. The results of most blood pregnancy tests take at least a
couple of days. The laboratory then advises the doctor of the result. Blood test results are about 99 % accurate and can detect lower amounts of hCG than urine pregnancy tests.
The two main types of blood pregnancy test include: 1. Quantitative blood test – measures the exact amount of hCG in the blood and can give an estimate how gestation is progessing
2.Qualitative blood test – only checks for the presence of hCG. Since this test
doesn’t measure the exact levels of hCG, it can’t offer an estimate of gestation
Urine pregnancy tests used by doctors
The doctor can give you a urine pregnancy test. You are asked
to urinate into a plastic cup or something similar. The doctor then tests the urine using a kit that may look similar to a home pregnancy test kit.
Inaccurate results from tests given by the doctor
Pregnancy tests by doctor are rarely inaccurate. The occasional error is usually due to mistakes made in the laboratory. However, you can be reassured that the pregnancy test taken by your doctor is much more likely to be accurate than a home test you perform yourself.
Other reasons for a missed period
Pregnancy is not the only reason for a missed period.
1. breastfeeding 2. emotional stress 3. severe weight loss 4. severe dieting and exercising 5. obesity 6. particular drugs 7. menopause onset.
عدل سابقا من قبل د.كمال سيد في الإثنين أغسطس 19, 2024 12:02 pm عدل 1 مرات
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Pregnancy stages and changes الأحد أغسطس 18, 2024 2:31 pm
Pregnancy stages and changes
Summary
Your body changes during pregnancy. You may love some changes and feel uncomfortable with others. You may experience of a lot of physical changes during pregnancy, or only a few. You will probably have emotional ups and downs during pregnancy. If you have depression or a mental health condition during pregnancy, you need specialist care and treatment. Some physical and emotional experiences are common to a particular trimester (stage) of pregnancy. If you are pregnant, your body is experiencing major change. From symptoms that you might expect, to ones that are completely unexpected, every woman will have a different pregnancy experience. It’s helpful to have an idea of how your body may react to the different stages of pregnancy. It also helps to know how pregnancy may affect your emotions and feelings.
Changes to your body that may indicate pregnancy
You may first realise that you’re pregnant when you miss your period. That’s a good time to take a pregnancy test or speak with your doctor.
Morning sickness
The first thing to know about morning sickness is that it can hit you at any time of day. Probably a result of your changing hormones, it usually starts about week 6 and settles by week 14. The good news is that you may feel better from morning sickness symptoms if you: drink small amounts of fluid, often. Try flat lemonade, sports drinks, diluted fruit juice, weak tea, clear soup or a hot drink made of stock suck on ice or ice-blocks (if you can’t keep down other fluids) try ginger tablets, dry ginger ale or ginger tea eat small amounts of food more often, so you don’t have an empty stomach eat a dry biscuit when you wake up in the morning, to avoid feeling sick when you get out of bed try salty foods such as potato crisps or salty biscuits suck on barley sugar or boiled lollies avoid fatty, rich or spicy foods avoid the smell of hot food avoid cooking dishes with strong smells rest as much as you can. A small percentage of pts have prolonged and excessive vomiting (called hyperemesis), which can lead to dehydration if it is not treated. See your doctor if you have severe morning sickness. In some extreme cases, women need to be rehydrated in hospital, using intravenous fluids
Pregnancy stages
We talk about 3 stages of pregnancy – first trimester, second trimester and third trimester. Some physical and emotional experiences are more common in each of these trimesters.. First trimester In the first trimester: You feel tired and possibly nauseous (like vomiting). You gain 1 or 2 kilograms, or maybe less if you have morning sickness. Most of this weight is in 1.the placenta (which feeds your baby) 2.breasts 3.uterus & the extra 4.blood that you are making. Your heartbeat and breathing rate are faster. Your breasts become tender, larger and heavier. Your growing uterus puts pressure on the bladder, so you feel needing to urinate (pee) a lot. You may feel swinging moods. You know exactly how you feel about having a baby, or you have no idea how to feel! Second trimester In the second trimester: You start to feel better, with less tiredness, morning sickness and moodiness. You may feel your mind is wandering and not focused at work or at home. You gain about 6 kilograms. You may feel anxious about tests (including an US) done at this stage. These tests will ensure you and your baby receive the right care. Your hair may become thicker and your fingernails may become stronger. Or, your nails may be softer and break more easily. You may crave some foods, such as sweet, spicy or fatty foods. You may not like the taste or smell of some foods. Quickening is when pt starts to feel baby's movement in the uterus. It feels like flutters, bubbles or tiny pulses. Quickening happens around 16 to 20 wks in pregnancy, but some pts may feel it sooner or later. Third trimester In the third trimester: Forgetfulness may continue. You feel tired and probably uncomfortable. You may be annoyed by the discomfort. You may start to worry about labour as it nears. You gain about 5 kilograms. Much of this weight is your 1.baby, also 2.amniotic fluid also 3.placenta 4.breasts 5.blood and 6.uterus. You may have back pain. You may find it hard to sleep because you are uncomfortable. The baby may be placingpressure on your lungs, making it harder to breathe. You may feel Braxton Hicks contractions (tightening of the muscles of the uterus). They do not mean labour is starting Remeberthe the hormone-induced fatigue, forgetfulness and moodiness
Depression during pregnancy
About 15 % of women will have depression or anxiety during pregnancy. And even more will suffer from these conditions after giving birth. Many women don’t seek help because they feel embarrassed or guilty about feeling so awful when are they are supposed to be happy. But depression is not something that you can
control in this way. Because an untreated mental health condition can have long term effects on your health
and wellbeing, and on your baby too, getting the right treatment is vital
Talk to your doctor if you are: *depressed or miserable for most of the day and on most days *annoyed, angry or anxious a lot of the time *crying a lot (and not always for a reason) *losing interest in activities that you usually like *struggling to sleep (even when your baby is sleeping), or sleeping more than usual *under- or over-eating *feeling tired most of the time *not able to concentrate *preoccupied or anxious about things going wrong with your pregnancy, you, your baby or your partner *feeling that you have not bonded with your baby, or that you have no maternal feelings *feeling guilty, or feeling that you are failing as a mother *thinking about harming yourself *thinking it would be better if you or your baby were dead *thinking about suicide. Remember, tell someone if you feel depressed, because early treatment is the best treatment. Plenty of safe and effective treatments are available for depression during pregnancy and while breastfeeding. But herbal and complementary treatments such as St John’s wort
may not be safe in pregnancy. Anxiety during pregnancy You may be feeling quite anxious about your pregnancy and about being a parent. Many pregnant women feel some anxiety, but a few develop an anxiety disorder that needs treatment. Symptoms of an anxiety disorder include: *constant worry, stress or nervousness *muscle tension and teeth clenching *not ever feeling calm *not being able to sleep well or for long *panic attacks. Other serious issues during pregnancy Some pregnant women develop mental health conditions that are a significant risk to
both them and their child. Other women may already have a mental health condition that is more difficult to manage during pregnancy. Specialist health care is needed for pregnant women with: *bipolar disorder (of which pregnancy may trigger the first episode), with manic highs and depression lows *schizophrenia *eating disorders, including anorexia nervosa and bulimia nervosa. The risks include a loss of nutrition for your baby, an increased risk of miscarriage, and anaemia
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Pregnancy ultrasound الأحد أغسطس 18, 2024 7:19 pm
Pregnancy ultrasound
Summary
US is used during pregnancy to 1.check the baby’s development 2.the presence of a multiple pregnancy and to help 3.pick up any abnormalities. US scan isn’t 100 per cent accurate, but its advantages are : 1.it’s non-invasive 2.painless and 3.safe for both mother and unborn baby 4.NON-radiaton. If fetal abnormalities are detected, further tests are offered to confirm the diagnosis, such as amniocentesis and chorionic villus sampling.
What is an ultrasound?
Ultrasound is a scan that uses high frequency sound waves to study internal body structures. The sound waves are emitted from a vibrating crystal in a handheld probe. The reflected sound waves or ‘echoes’ are then translated into a grainy, two-dimensional or sometimes three-dimensiona image on a monitor. Ultrasound is used during pregnancy to check the baby’s development and to help pick up any abnormalities such as Down syndrome. Since the procedure can’t produce high quality images, any suspected abnormalities need to be confirmed with other tests. Uses of the ultrasound US may be used at various points during pregnancy, including: First trimester US is performed within the 1ST 3 months gestation : 1. To check that the embryo is developing inside the uterus & not in a fallopian tube or other 2.To confirm the number of embryos 3.calculate the gestational age and 4.Estimate the baby’s due date. :Second trimester US is performed b/w wks 18 and 20 to 1. check the development of fetal structures such as the spine, limbs, brain & internal organs To check The size and location of the placenta .2. Make sure the location of thePlacenta is not blocking the CX .3. To establish the baby’s sex can be established, if the parents wish to know .4. Third trimester US is performed after 30 wks to check that the baby is continuing to grow at a normal rate. Medical issues to consider US is a safe, painless and non-invasive procedure. Many parents consider the US as an opportunity to see their unborn child, and perhaps discover its sex. However, you should remember that the US is a diagnostic procedure and, in some cases, it may suggest that a fetus has an abnormality. Further tests are usually needed to confirm the diagnosis. Ultrasound procedure The procedure depends on the type of ultrasound used, but may include: Trans-abdominal US – sound waves pass very well through water. Full bladder is used as a ‘porthole’ (window) to the uterus, so you have to drink plenty of water before the test. YU lie supine facing sonographer at yur RT side. Gel is applied to abdomen (to provide better contact between your skin and probe) Sonographer moves the scanner in various positions. Pictures are sent instantly to a nearby monitor. Sonographer may have to push firmly at times in order to see the deeper structures. The scan usually takes about 30 minutes. Vaginal US – in some cases, a transabdominal US can’t produce clear enough pictures. There may be too much air in your bowel, for instance, and air is a poor conductor of sound waves. In these cases, a Transvaginal probe is inserted into your vagina. The scan usually takes about 30 minutes. Immediately after the ultrasound Once the US is finished, sonographer wipes away the gel, and you can go to the toilet. The report is sent to your doctor, so you will have to make an appointment to get the result. Possible complications There are no known risks, complications or side effects for either the mother or her unborn baby. Taking care of yourself at home An US scan is safe, painless and non-invasive, so there is no need to take any special precautions afterward. You are free to go about your normal business. Long term outlook What happens next depends on the results of your US. Note that a normal result doesn’t guarantee that your baby is normal, because some abnormalities cannot be found using this test. If fetal abnormalities were detected, you may need further tests to confirm the diagnosis. These tests, including amniocentesis and chorionic villus sampling, are optional. Discuss the benefits, risks and complications of these tests with your doctor before deciding whether or not to go ahead. Other types of pregnancy US tests Other types of pregnancy tests you may be offered could include: Amniocentesis – a small amount of amniotic fluid is taken using a slender needle inserted through the abdomen. The needle is guided with the help of US. The fluid sample contains cells, which are then examined in a laboratory for chromosomal abnormalities. The risk of miscarriage following amniocentesis is around one in 250. Chorionic villus sampling – a slender needle is inserted through the abdomen OR cervix to take a small sample of placenta. The needle is guided with the help of US. The chorionic villi are then tested in the laboratory for chromosomal abnormalities. The risk of miscarriage following chorionic villus sampling is one in 100.
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Normal early pregnancy US الإثنين أغسطس 19, 2024 12:50 pm
Fertilization (conception or impregnation or insemiation) { During ovulation, an egg travels from an ovary down a fallopian tube to prepare for fertilization with sperm.} egg and sperm meet in the fallopian tube where the sperm start to digest the sticky cells. While it takes only one sperm to make a baby, several need to attach to the outer shell and the membrane of the egg before one can enter and fertilise it. A man may ejaculate 40 million to 150 million sperm, which start swimming upstream toward the fallopian tubes on their mission to fertilize an egg. Fast-swimming sperm can reach the egg in a half an hour; others may take days. The sperm can live up to 48-72 hours.Oct 11, 2023 After ovulation the egg lives for 12 to 24 hours and must be fertilised in that time if a woman is to become pregnant. Fertilization is a complex multi-step process that is complete in 24 hours The sperm from a male meets an ovum from a female and forms a zygote; this is the point in which pregnancy begins and leads to a 280-day journey for a female. There are two ways to track this process, and they differ by the day counting begins Fertilization, simply, is the joining of an egg and a sperm. It happens inside a female reproductive system and is the first step of a pregnancy. It specifically involves the joining of the female reproductive cells (egg) with the male reproductive cell (sperm). The events of conception usually include 4 stages: (1) contact and recognition between sperm and egg; (2) regulation of sperm entry into the egg; (3) fusion of genetic material from the two gametes; (4) activation of egg metabolism to start development. A pregnancy starts with fertilization, when a woman's egg joins with a man's sperm. Fertilization usually takes place in a fallopian tube that links an ovary to the uterus. If the fertilized egg successfully travels down the fallopian tube and implants in the uterus, an embryo starts growing. Fertilisation: The fusion of a haploid male gamete (spermatozoa) and a haploid
female gamete (ovum) to form a diploid cell, the zygote, is called fertilization. Within 24 hours of ovulation,Sperm fertilizes an egg (conception occurs). About six days after fertilization: The fertilized egg implants into uterine lining. Around day 21: If conception and implantation occurred during this menstrual cycle, you're pregnant. Fertilization of the ovum begins in the fallopian tube, & starts cell division as it moves down the fallopian tube Once in the uterine cavity, it digs a hole & burries itself eccentrically into the endometrium and covers itself over This is the 1ST sign we see in us, called Intradecidual Sac sign (IDSS):/1
1. IDSSisseen by TVS at 4-4.5 wks after LMP
2.Seen on US as a small cyst ~ 2 mm or more
3. Located eccentric to the central echogenic line 4. Has Thin echogenic Rim around NB:In principle, the central echogenic line represents the uterine cavity the outer lines represent the basal layer of the endometrium or the interface between the endometrium and the myometrium Pitfalls (some confusing Mimicks for IDSS) such as : Intracavitory fluid, which indicates endometrial cyst, which is usually located in the endometrial/myometrial junction; However IDSS is A/close to the central white line & has B/little color flash beside 2/ THE 2ND sonographic sign :As the GS continues to grow we get the Double Decidual Sac Sign (DDSS) 1. The decidua is the enometrium of the 1ST trimester 2. Seen by 5 wks 3. Seen as rounded OR oval fluid collection 4. Surrounded by 2 echogenic rings: A/Outer decidua (is the decidualized endometrium) B/inner chorion Pitfalls (some confusing Mimicks for DDSS) such as : Pseudo Gestational sac 1. Occurs in 10-20%of Ectopic pregnancies 2. Fluid OR blood from tube, accumulate in endometrial cavity 3. US appearance : A/ Fluid collection B/ Has acute angles OR Tear-drop shape C/ It has an echogenic Rim, around which is D/ the endometrium Important Message : Any rounded or oval fluid collection in a woman with positive pregnancy test most likely represent an intra-uterine Gestational sac 3/The 3RD visible milestone sonographically is the Yolk sac (YS) 1. Seen at 5.5 wks 2. The presence of a yolk sac within a gestational sac confirms IUP 3. The YS has a *thin smooth outline, with a *spherical shape *rounded Ring-like 4.structure *3-5 mm & *Should NEVER be more than 5 mm 5. Calcified or thick-wall YS is abnormal and may be asspciated with pregnancy failure
6. Plays a critical role in embryonic development by providing nutrients * visualization of YS is useful in distinguishing IUP from a pseudogestational sac.
7. The number of Yolk sacs, is equal to the number of amnions (In multiple gestation, count the yolk sacs to determine amnionicity) 8. Becomes obliterated as amnion fuses with chorion at 14-16 wks 4/ The 4TH visible sonographic sign of pregnancy is the Embryo which is seen at 6-6.5 wks 1. embryo appears like a little dot On the YS, the Diamod-Ring sign where the diamond is the embryo, & the ring is the YS
2.cardiac activity my be seen as a flickering in this areabefore the embryo is suficiently large enough to allow accurate measurement of length
3.Once the embryo is discretely resolved, longest axis is measured & referred to as the Crown Rump Length {CRL} 5/Amnion The 5TH visible sonographic pregnancy sign 1. Seen closer to 7 wks. 2. As the embryo enlarges, the Amnion becomes visible surrounding the embryo 3. The embryois in the Amniotic cavity .4 The yolk sacis in the chorionic cavity 5. At 7-9 wks, the Amnion is expanding & the YS is now free floating out in the chorionic cavity 6. As continuous growth & development progress, the embryo visibly changes from a "dot" to a "grain of rice" size, to a more "kidney bean" shaped structure
7. The embryo now is Renamed a Fetus at 10 wks 8. By the end of the 1ST trimester : The 1ST trimester of pregnancy is counted from the first day of LMP through to wk 12. *Organogenesis is complete * The Amnion is getting closer to the chorion But doesn't fuse until 14-16 wks








 الجمعة أغسطس 02, 2024 12:22 pm
الجمعة أغسطس 02, 2024 12:22 pm