
موقع د. كمال سيد الدراوي
طبي_ اكاديمي _ ثقافي _ تعليمي _ _ استشارات طبية_فيديو طبي
|
| | | UTERUS & OVARIES |  |
| | |
| كاتب الموضوع | رسالة |
|---|
د.كمال سيد
Admin




عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس : 
علم بلدك : 
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي : 
|  موضوع: رد: UTERUS & OVARIES موضوع: رد: UTERUS & OVARIES  الأربعاء أبريل 24, 2024 5:33 pm الأربعاء أبريل 24, 2024 5:33 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:35 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:38 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:41 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:43 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:44 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:46 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:49 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:50 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:53 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:55 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 5:56 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: OVARIN CYSTS الأربعاء أبريل 24, 2024 6:51 pm | |
| Benign Ovarian Cysts• Functional Cysts • Follicular • Corpus Luteal • Hemorrhagic Cysts • Theca-luteal Cysts • Postmenopausal Cysts • Endometriomas PathologySmall cystic ovarian structures should be considered normal ovarian follicles unless the patient is pre-pubertal, post-menopausal, pregnant, or the mean diameter is >3 cm (see the 1-2-3 rule). Types of cystsfunctional cysts (can produce hormones):
follicular cysts of the ovary (estrogen): >3 cm
corpus luteum cysts (progesterone)
theca lutein cyst: gestational trophoblastic disease
complications in functional cysts:
hemorrhagic ovarian cyst
enlargement
rupture
torsion
other cysts:
multiple large ovarian cysts in ovarian hyperstimulation syndrome
postmenopausal cyst: serous inclusion cysts of the ovary
polycystic ovaries
ovarian torsion
ovarian cystic neoplasm
Radiographic featuresUltrasound is usually the first imaging modality for assessment of ovarian lesions. Imaging features of simple ovarian cysts: A cyst may become large enough to obscure the ovary from which it is arising. Radiology reportThe Society of Radiologists in Ultrasound made in 2019 the following recommendations regarding reporting of simple adnexal cysts of suspected ovarian origin based on size and menopausal status 2: - premenopausal women
- less than 3 cm: no need to report; if described, consider calling a "follicle" rather than a "cyst" to reduce patient anxiety
- impression: normal ovaries/adnexa
- recommendation: no follow-up
more than 3 to ≤5 cm: report presence of simple cyst(s) and largest cyst diameter
impression: benign finding in the physiologic size range
recommendation: no follow-up
more than 5 cm: report with all cyst diameters
impression: benign simple cyst
recommendation:
more than 5 cm to ≤7 cm: follow-up either in 2-6 months for resolution/re-characterization or in 6-12 months for growth rate assessment, but no follow up is needed if the cyst is exceptionally well-visualized/characterized and documented with confidence by the imager
more than 7 cm: follow-up either in 2-6 months for resolution/re-characterization or in 6-12 months for growth rate assessment
follow-up of cyst (previously >5 cm): describe in report with all cyst diameters if not resolved
a) is it decreased in size
impression: benign inconsequential finding; decrease in size excludes neoplasm
recommendation: no further follow-up needed
b) is it similar in size
impression: benign simple cyst with stability over ≥12 months, most likely nonneoplastic or very slow growing benign neoplasm
recommendation: follow-up at 2 years from initial study to document stability and understand growth rate
c) is it increased in size
impression: enlarging simple cyst, most likely a benign neoplasm
recommendation: follow-up in 1 year to evaluate any further changes in size
next
https://radiopaedia.org/articles/ovarian-cyst-2
| |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الأربعاء أبريل 24, 2024 7:27 pm | |
| - postmenopausal women
- less than 1 cm: no need to report
- impression: normal ovaries/adnexa
- recommendation: no follow-up
more than 1 cm to ≤3 cm: report presence of simple cyst(s) and largest cyst diameter
impression: benign inconsequential finding
recommendation: no follow-up
more than cm: report with all cyst diameters
impression: benign simple cyst
recommendation:
more than 3 cm to ≤5 cm: follow-up either in 3-6 months for resolution/re-characterization or in 6-12 months for growth rate assessment, but no follow up is needed if the cyst is exceptionally well-visualized/characterized and documented with confidence by the imager
more than 5 cm: follow-up either in 3-6 months for resolution/re-characterization or in 6-12 months for growth rate assessment
follow-up of cyst (previously >3 cm): describe in report with all largest cyst diameters if not resolved
a) is it decreased in size
impression: benign simple cyst; decrease in size excludes neoplasm
recommendation: no further follow-up needed
b) is it similar in size
impression: benign simple cyst
recommendation: follow-up at 2 years from initial study to document stability
c) is it increased in size
impression: enlarging simple cyst, most likely a benign neoplasm
recommendation: follow-up in 1 year to evaluate any further changes in size
Note that these guidelines do not apply to hemorrhagic ovarian cysts. Treatment and prognosis | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الخميس أبريل 25, 2024 11:40 am | |
| Ovarian follicle An ovarian follicle (also known as a Graafian follicle in its mature state) is the basic unit of female reproductive biology and is composed of 1/ roughly spherical aggregations of cells 2/ and contains a single oocyte. Gross anatomyAn ovarian follicle can be initiated to grow and develop, culminating in ovulation of usually a single competent oocyte in humans. Approximately 10 ovarian follicles begin to mature during a normal menstrual cycle and out of these usually one will turn into a dominant ovarian follicle. Ovulation is when a mature egg is released from an ovary and moves along a fallopian tube towards the uterus. This usually happens once each month, about two weeks before next period. Ovulation can last from 16 to 32 hours. During ovulation, 1/ the =primary-follicle&lang=us]primary follicle forms the =secondary-follicle&lang=us]secondary follicle 2/ and then the =mature-vesicular-follicle&lang=us]mature vesicular follicle. After rupture, 3/ the follicle turns into a corpus luteum and eventually 4/ involutes to the corpus albicans. Radiographic featuresUltrasoundFollowing maturations under the development of gonadotropins, small follicles can be seen as small sonolucent rounded structures around the ovary. In the normal physiological state one of the follicles enlarges to ~1 cm to become a dominant follicle which grows further to ~2.5 cm 1. This is then called an ovarian follicular cystSee the 1-2-3 rule.The 1-2-3 rule is a simple aide-mémoire describing the nomenclature of any small simple anechoic structure in the ovary on ultrasound: <1 cm = follicle. 1-2 cm = dominant follicle. >3 cm = cyst. MRI Ovarian follicles, as well as follicular cysts, may be seen as rounded structures around the ovary. Signal characteristics - T2: high signal (as with many fluid-filled entities) 7
History and etymologyIt (the Graafian follicle) is named after Reinier de Graaf (1641-1673), a Dutch physician and anatomist a follicular cyst occurs when follicle continues o grow.. it is a simple thin wall simple small cyst filled with clear fluid, no septa ,no debris, no calcification,no solid component seen.. there is no internl vasculation.. cysts ranging from 31 to 38 mm are not serious & can resolve spontaneously without any complications & no need for surgery.. sometimes a cyst grows & become a large ovarian cyst which needs follow up consultation . KAMALSAYED
عدل سابقا من قبل د.كمال سيد في الخميس أبريل 25, 2024 12:06 pm عدل 2 مرات | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الخميس أبريل 25, 2024 11:44 am | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الخميس أبريل 25, 2024 11:45 am | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الخميس أبريل 25, 2024 11:47 am | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: adnexa الخميس أبريل 25, 2024 12:37 pm | |
| AdnexaAdnexa is a Latin word meaning attachment or appendages. It refers to the 1/ ovaries, 2/ fallopian tubes, and 3/ ligaments that hold the reproductive organs in place. These are all located in your lower abdomen near your pelvic bone. functionThe adnexal area is made up of a series of ligaments that collectively support and keep the uterus in the correct orientation as it grows during pregnancy. The broad ligament also contains the blood supply to the uterus and the ovary .The adnexa lie between lateral margins of the uterus and pelvic side wall During adulthood, ovaries reach an average size of 3.5 x 2 x 1 cm, equivalent to a volume of between 3 and 6 ml. Over time, the eggs in the ovaries decrease and ovulations eventually cease .normal ovarian are cysts that form during your monthly menstrual cycle, called functional cysts. Functional cysts are not the same as cysts caused by cancer or other diseases. The formation of these cysts is a perfectly normal event and is a sign that the ovaries are working well .In general, an enlargement of the ovary cyst beyond 4 cm can cause persistent discomfort. It would, therefore, alert a patient and their doctor of a possible problem. It is critical to follow these ovarian cysts to rule out possible conditions such as endometriosis or ovarian cancer. In postmenopausal women, simple cysts greater than 1 cm in size should be described but do not need follow-up imaging unless they are greater than 3–5 cm, using the higher threshold for exceptionally well-visualized simple cysts. These thresholds are greater than 3 cm and greater than 5–7 cm in premenopausal women. The fallopian tubes and ovaries are jointly referred to as the uterine adnexa (appendages). This is where the term adnexitis originates for inflammation of the fallopian tubes and of the ovaries. Inflammation of the fallopian tubes alone is known as salpingitis. Polycystic ovaries (PCO) are described on ultrasound scan as the "presence of 12 or more follicles in each ovary measuring 2-9 mm in diameter, and/or increased ovarian volume (>10 ml)" 1 . https://www.google.com/search?client=firefox-b-d&q=adnexa+ultrasound+normal#ip=1
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 4:05 pm عدل 1 مرات | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الخميس أبريل 25, 2024 12:39 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الخميس أبريل 25, 2024 1:42 pm | |
| Benign Ovarian Cysts
• functionall Cysts
• @Follicular
• @Corpus Luteal
• @Hemorrhagic Cysts
• @Theca-luteal Cysts
• Postmenopausal Cysts
• Endometriomas
Follicular cyst
Result of mature follicle failing to ovulate or involute;
Cyst must be > than 2.5 cm; usually regress on own
Corpus Luteal Cyst
Result from failure of absorption or from excess
bleeding into the corpus luteum
Have thicker walls with crenulated appearance
Hemorrhagic cysts
• Internal hemorrhage from granulose
cells lining functional or corpus lutealcysts
• Appearance depends on age and
amount of hemorrhage ranging from
hyperechoic with posterior acoustic
enhancement to reticular pattern
with internal echoes to fluid-fluid line
• No flow seen within cyst on Doppler
Acute hemorrhagic cyst
Echogenic free fluid in pelvis indicates a leaking
or ruptured cyst –woman with these cysts
complain of pelvic pain
Hemorrhagic Cysts
Septations with internal echoes and no flow
Theca-luteal cysts
• Largest of functional cysts
• Associated with high levels of HCG
• Seen in gestational trophoblastic
disease and ovarian hyperstimulation
syndrome with infertility drug
therapy
• These cysts are bilateral, multilocular
and very large | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Ovary الجمعة أبريل 26, 2024 1:14 pm | |
| OVARYThe human OVARY consists of an inner medulla and outer cortex with indistinct boundaries. The medulla contains the blood vessels and nerves, while the cortex is occupied by developing follicles. A cross-section of an ovary will reveal follicles in various stages of development. In a normal menstrual cycle one follicle will grow containing one egg. The follicle will get bigger until it ruptures at ovulation which then releases the egg. This is usually around 14 days after the beginning of the menstrual cycle
The average follicle is said to develop at a rate of 2.7 mm/day. but this may vary from 2 to 5 mm/day or even no growth over the 3–4 days preceding ovulation higher pregnancy rates were achieved when the leading follicles were in the 23 to 28 mm range. In some situations, one follicle is enough for pregnancy, but if you have trouble conceiving, then getting the right medical advice on increasing your follicular count might actually help. Some infertility treatments help in increasing this count and raise your chances of pregnancy regardless of your age Depending on the number of antral follicles, a woman is considered to have adequate or normal ovarian reserve if the count is 6-10. Low ovarian reserve, if the count is less than 6 ovarian reserve and high ovarian reserve if is greater than 12. There are a number of factors that can contribute to slow growing follicles, including 1/age, 2/ high FSH levels, 3/ poor ovarian blood flow, 4/ insulin resistance, 5/ thyroid problems, 6/ PCOS, 7/ endometriosis, 8/ certain medications, 9/ environmental toxins, 10/ and stress . Primordial follicles begin to form at 15 weeks of intrauterine gestation, and at birth, the fetal ovary on an average contains ∼400 000 primordial follicles. BUT only about 400 will be recruited for potential ovulation and fertilization during a woman's reproductive yearsAn ovarian follicle (also known as a Graafian follicle when it is in its mature state) is the basic unit of female reproductive biology and is composed of roughly 1/spherical aggregations of cells 2/and contains a single oocyteAn ovarian follicle can be initiated to grow and develop, culminating in ovulation of usually a single competent oocyte in humans. stages of follicle developmentFollicles during the folliculogenesis process can be divided into three stages: 1/primordial follicles (PmF), 2/growing follicles, 3/and Graafian follicles (GF). Growing follicles can be further divided into 1/primary follicles (PrF) and 2/secondary follicles (SF). The primordial follicles are 1/ oocytes surrounded by less differentiated squamous granulosa cells 2/ and are derived from oocyte nests. The primary follicles are oocytes surrounded by a single layer of cuboidal granulosa cells that have initiated follicle development.  Approximately 10 ovarian follicles begin to mature during a normal menstrual cycle and out of these usually one will turn into a dominant ovarian follicle During ovulation, the =primary-follicle&lang=us]primary follicle forms the =secondary-follicle&lang=us]secondary follicle and then the =mature-vesicular-follicle&lang=us]mature vesicular follicle. After rupture, the follicle turns into a corpus luteum and eventually involutes to the corpus albicans. A dominant ovarian follicle refers to the follicle that enlarges to release an ovum during a menstural cycle. Usually approximately 10 Graafian follicles begin to mature where one becomes a dominant follicle and the rest become =atretic-ovarian-follicles&lang=us]atretic ovarian follicles. After release of the ovum the remainder of the dominant follicle turns into a corpus luteum and finally into a scarred corpus albicans. On occasion there can be two or more dominant follicles. Generally the accepted ultrasound size cut off for a dominant follicle is between 1-2 cm
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 4:11 pm عدل 1 مرات | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الجمعة أبريل 26, 2024 5:26 pm | |
| Ovulation
After rupture, the follicle turns into a corpus luteum and eventually involutes to the corpus albicans The corpus luteum (plural: corpora lutea) is a temporary endocrine structure involved in ovulation and early pregnancy.During ovulation, the primary follicle forms the secondary follicle and subsequently the mature vesicular follicle. At ovulation ovulation the follicle ruptures expelling the ovum into the fallopian tube. The remnants of the follicle after ovulation is referred to as the corpus luteum and ranges from 2-5 cm in diameter but involutes as it matures. The corpus luteum produces estrogen and progesterone, maintaining optimum conditions for implantation if the ovum is fertilised: - IF ovum fertilised : the corpus luteum continues to produce these hormones and maximizes the chance of implantation into the endometrium; it reaches a maximum size at ~10 weeks and finally resolves at around 16-20 weeks
- IF ovum NOT fertilised: the corpus luteum involutes and turns into a corpus albicans by around 2 weeks
In some instances (especially in twin pregnancies), there may be more than one corpus luteum - (e.g. two corpora lutea) Radiographic featuresUltrasoundThe corpus luteum is 1/ a thick walled cyst with characteristic 2/ " ring of fire" peripheral vascularity. 3/ It usually has a crenulated inner margin 4/ and internal echoes. Differential diagnosisGeneral considerations include: - adnexal ectopic pregnancy
- ectopic pregnancy is more echogenic than the ovary in 77-88% 5
- corpus luteum is more echogenic than the ovary in ~3% 5
ovarian neoplasm
History and etymologyThe term "corpus luteum" is derived from the Latin meaning "yellow body" where "corpus" means body and "luteum" means yellow . The corpus luteum eventually involutes into the " corpus albicans" ("white body"). - corpus luteum cyst
- The corpus albicans is a fibrous scar that results from the involution of the corpus luteum if fertilisation does not occur. When seen on ultrasound, it is 1/ a small,2/ lobulated 3/ echogenic 4/ intra-ovarian lesion.
History and etymologyIt is Latin for "whitening body", after the white appearance of the fibrous tissue
 MRI corpus luteam 
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 4:22 pm عدل 1 مرات | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: رد: UTERUS & OVARIES الجمعة أبريل 26, 2024 6:33 pm | |
| Fallopian tube The fallopian tube ( TA: tuba uterina 8), also known as the uterine tube or ( salpinges), less commonly, the oviduct, is a paired hollow tube that bridges the ovary and uterus and functions to convey the mature ovum from the former to the latter. If conception occurs, it usually does so within the tube, which can be affected by a wide range of pathology. Gross anatomyThe fallopian tube is approximately 10-12 cm long and 1-4 mm in diameter. It courses between the ovary laterally and the uterus medially. Through it, the ovum passes into the uterine cavity. The peritoneal reflection draping over the salpinges forms the mesosalpinx. The fallopian tube can be divided into five anatomic segments ( from lateral to medial, the path that an ovum takes after ovulation): - fimbriae: ~25 finger-like projections that drape over the ovary
- the ovarian fimbriae are longer than the others and are attached to the tubal pole of the ovary
infundibulum: a funnel-shaped lateral part that drapes over the ovary. the fimbriae emanating from it
it opens into the peritoneal cavity at the abdominal ostium
ampulla: the widest and longest section, forming over half the length, it is the most established location of fertilisation
isthmus: immediately lateral to the uterus, it is the narrowest segment, as its name suggests.
interstitial or intramural segment: the section within the myometrium
See mnemonic hereA useful mnemonic to remember the order of the five segments of the fallopian tube, from lateral to medial, the direction an ovum would pass following ovulation, is: - Four INches Across IS IMpossible
Four inches (10 cm) is the approximate length of the fallopian tube. Mnemonic- F: fimbriae
- IN: infundibulum
- A: ampulla
- IS: isthmus
- IM: intramural (interstitial)
RelationsThe extrauterine part of the fallopian tube courses between the two folds of the broad ligament at its superior aspect 5. - at its medial end, the interstitial segment is continuous with the uterotubal junction, a continuation of the endometrial cavity
- at its lateral end, the infundibulum opens into the peritoneal cavity
The fallopian tubes are one of the components of the adnexa. Arterial supplyVenous drainage- lateral one-third via the pampiniform plexus to the ovarian veins
- medial two-thirds via the uterine plexus to the internal iliac vein
Lymphatic drainage- via ovarian vessels to the para-aortic nodes and uterine vessels to the internal iliac chain
- some drainage also to the inguinal nodes via the round ligament
InnervationVariant anatomy- absent unilateral
- hypoplastic unilateral
- hypoplastic bilateral
- abnormal entry into uterine body or fundus
HistologyLike many other muscular hollow tubes, it has two layers of muscle ( inner circular, outer longitudinal) and is lined by a mixture of ciliated and non-ciliated =columnar-epithelium&lang=us]columnar epithelium. It is the former that pushes the ovum towards the uterus. Radiographic featuresThe normal fallopian tube is not visualized at cross-sectional imaging unless it is outlined by fluid. In the presence of peritoneal fluid or contrast material, the fallopian tubes appear as paired, thin, serpentine juxtauterine structures extending either anteriorly or posteriorly into the cul-de-sac Fluoroscopy Contrast studies can be completed by performing a hysterosalpingogram (HSG). History and etymologyThe fallopian tube is named after Gabriel Fallopio (1523-1562), an Italian anatomist. He is the same anatomist who gave his name to the fallopian ligament and the fallopian canal. Despite the eponym, the word "fallopian" is usually rendered in lowercase as it is an adjectival form derived from a name, not the name itself (cf. nabothian) 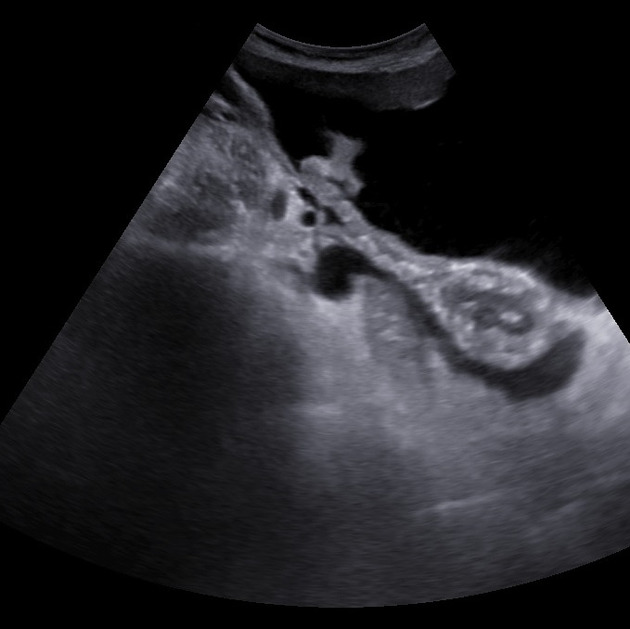
Related pathologyhematosalpinx
hydrosalpinx
pyosalpinx
Quiz questions | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2464
نقاط : 4252
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Urinary bladder السبت أبريل 27, 2024 11:11 am | |
| Urinary bladderThe urinary bladder (more commonly just called the bladder) is a distal part of the urinary tract and is an extraperitoneal structure located in the true pelvis 6. Its primary function is as a reservoir for urine The pelvic outlet also called the inferior pelvic aperture, defines the lower margin of the lesser (true) pelvis. The pelvic cavity (the true pelvis) predominantly contains 1/ the urinary bladder,2/ the colon, and 3/ the internal reproductive organs. This space is enclosed between the pelvic inlet and the pelvic outlet. Gross anatomyThe bladder has 1/ a triangular shape with 2/ a posterior base ( fundus), 3/ superior dome, 4/ anterior apex, and 5/ an inferior neck with 6/ two inferolateral surfaces 6. 7/ It is lined with a rough, trabeculated transitional cell epithelium, except at the trigone 6. The apex (anterior) of the bladder is directed behind the symphysis pubis 6, connected to the anterior abdominal wall and umbilicus through the median umbilical ligament (remnant of the embryological urachus) 6, which is covered by the median umbilical fold formed by the overlying peritoneum. The trigone is a triangular area of smooth mucosa lined by stratified squamous epithelium on the internal surface of the base. The superolateral angles are formed by the ureteric orifices and the inferior angle is formed by the internal urethral orifice. As men age, the trigone overlying the mid-portion of the central zone of the prostate may start to protrude as the prostate enlarges forming a mild hemispherical elevation proximal to the internal urinary sphincter, which is called the uvula of the bladder .The urethra arises from the neck of the bladder and is surrounded by the internal urethral sphincter. The urethra is separated from the symphysis pubis by retropubic fatty space of Retzius . As the bladder fills with urine it becomes ovoid and extends superiorly into the abdominal cavity Contraction is facilitated by the detrusor muscle The peritoneum over the bladder is relatively loose except at the insertion points of the ureters at the posterior bladder and at the inferior bladder where the peritoneum condensed into pelvic fascia and attached to the pubic bone (pubovesical ligament in females and puboprostatic ligament in males), lateral walls of pelvis and rectum. This makes the inferior part of the bladder relatively fixed. In males, the peritoenum is reflected between the rectum and bladder to form the rectovesical pouch. In females, there are two reflections namely rectouterine pouch (pouch of Douglas) and vesicouterine pouch . Arterial supply upper part in both males and females: superior vesical artery lower part: males: inferior vesical artery females: vaginal artery All of which are branches from the anterior division of the internal iliac artery Venous drainagemale: vesical and prostatic venous plexus via similarly named veins to the internal iliac veins and internal vertebral veins
female: vesical and uterovaginal plexuses draining into the internal iliac veins
Lymphatic drainage
upper part: lymphatic vessels pass to external iliac lymph nodes
lower part: lymphatic vessels pass to internal iliac lymph nodes
Innervation
autonomic innervation from the vesical nerve plexuses (composed of sympathetic and parasympathetic nerve fibers) sympathetic: reach the pelvic and subsequently the vesical plexus via hypogastric nerves (from the inferior mesenteric ganglion which in turn is supplied by the lumbar splanchnic nerves from the sympathetic lumbar outflow) parasympathetic: reach the pelvic and subsequently the vesical plexus via pelvic splanchnic nerves (from the parasympathetic sacral outflow) somatic innervation is via the pudendal nerves the hypogastric, pelvic splanchnic and pudendal nerves all have afferent components For an account of the functional anatomy of micturition, refer to bladder neuroanatomy
Relations - male
anteriorly : pubic symphysis
posteriorly : rectovesical pouch and rectum
inferiorly : obturator internus muscle, levator ani muscle, prostate (anterior to posterior) 6
superiorly : peritoneum
laterally : ischioanal fossa
Relations - female
anteriorly : pubic symphysis
posteriorly : vesicouterine pouch, uterus, cervix, vagina inferiorly : urogenital diaphragm, pelvic fascia, perineal membrane
superiorly : uterus, peritoneum
laterally : ischioanal fossa
Variant anatomy
double bladder: receives ipsilateral ureter and has a separate urethra
septation: septum may divide the bladder internally into two or more compartments
agenesis: persistence of the cloaca
ureterocele: dilation of the intravesical part of the ureter
The bladder is usually easier to evaluate when full, and it is sometimes difficult to identify when empty. Plain radiographs The bladder may be seen as a rounded soft tissue mass . Fluoroscopy Cystography can be performed where the bladder is filled with contrast either via an antegrade or retrograde technique. UltrasoundThe bladder wall is best assessed with this modality - it should not exceed 3-5 mm in thickness. Ureteric jets can be assessed using color Doppler ultrasound 1. MRIT1: bladder wall and contents are homogeneous low signal
1 T2: bladder wall is of low signal and urine of high signal, allowing for a contrast between the two
Related pathology
signs
pine cone bladder or Christmas tree bladder
thimble bladder
gamuts
bladder wall calcification
trauma
urinary bladder rupture
neoplastic
bladder cancer
transitional cell carcinoma
squamous cell carcinoma
others
urinary bladder diverticulum
urinary bladder hernia
ketamine bladder
Quiz questions 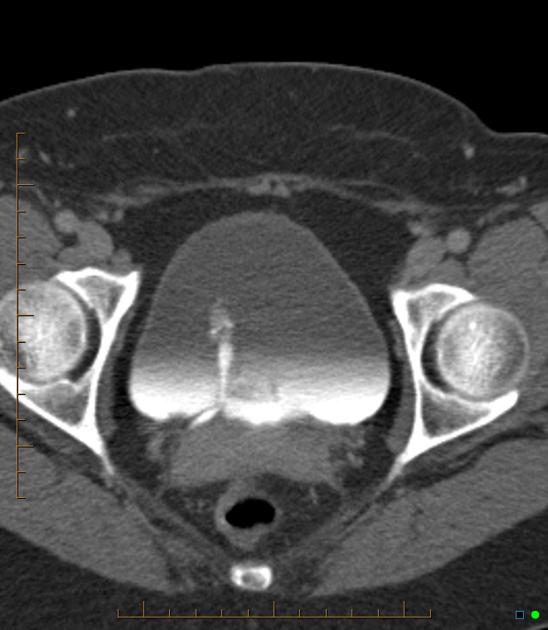 ureteric jet  normal bladder on cystography https://radiopaedia.org/articles/urinary-bladder?lang=us
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 4:45 pm عدل 1 مرات | |
| | | | | | UTERUS & OVARIES | |
|
مواضيع مماثلة | |
|
| | صلاحيات هذا المنتدى: | لاتستطيع الرد على المواضيع في هذا المنتدى
| |
| |
| |
|


