The Porta hepatis, also known as the transverse hepatic fissure, (is the gateway to the liver) is a deep fissures in the inferior surface of the liver through which all the neurovascular structures (except hepatic veins) and also hepatic duct enter or leave the liver It runs in the hepatoduodenal ligament and contains
عدل سابقا من قبل د.كمال سيد في الإثنين أبريل 15, 2024 11:18 am عدل 3 مرات
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: porta hepatis السبت أبريل 13, 2024 7:00 pm
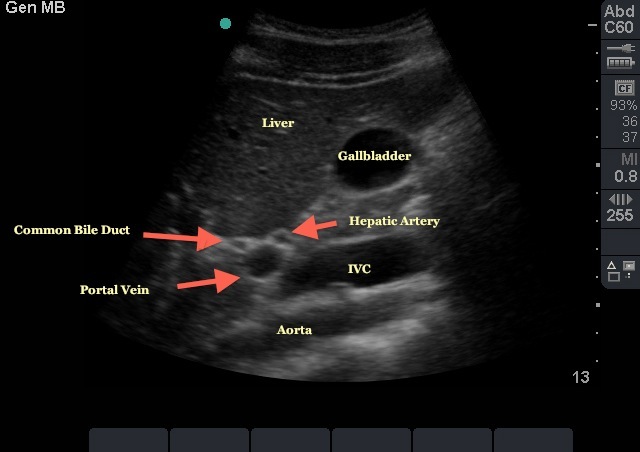
PORTA HEPATIS The arrangement of structures around the porta hepatis can be described by the letter "H". The left limb of the "H" is formed by ligamentum venosum superiorly and ligamentum teres inferiorly. Meanwhile, the right limb is formed by the inferior vena cava (IVC) superiorly and the gall bladder inferiorly. The crossbar of the letter "H" is the porta hepatis where the bile ducts, hepatic arteries, and portal vein enters and exits the region. There are also some nerves and lymphatics in the porta hepatis 5. The area bounded between the gall bladder and ligamentum teres is the quadrate lobe of the liver while the area bound between ligamentum venosum and IVC is the caudate lobe of the liver 5. From anterior to posterior, these porta hepatis structures lie in the order of duct-artery-vein thus the hepatic ducts are more accessible in surgery. The porta hepatis provides attachment for the lesser omentum. It lies between caudate lobe posteriorly and quadrate lobe anteriorly.
porta hepatitis with choledocholithiasis Figure 1: porta hepatitis
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 7:03 pm عدل 1 مرات
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: liver lobes السبت أبريل 13, 2024 7:31 pm
LIVER LOBES
The Caudate lobe (posterior hepatic segment I) is situated upon the posterosuperior surface of the liver on the right lobe of the liver, opposite the tenth and eleventh thoracic vertebrae . The liver is divided into four lobes. This image shows the large right lobe and a smaller left lobe separated by the falciform ligament. In human anatomy, the liver is divided grossly into four parts or lobes: the right lobe, the left lobe, the caudate lobe, and the quadrate lobe. Seen from the front – the diaphragmatic surface – the liver is divided into two lobes: the right lobe and the left lobe. Viewed from the underside – the visceral surface – the other two smaller lobes, the caudate lobe and the quadrate lobe, are also visible.[1] The two smaller lobes, the caudate lobe and the quadrate lobe, are known as superficial or accessory lobes, and both are located on the underside of the right lobe.[2] The falciform ligament, visible on the front of the liver, makes a superficial division of the right and left lobes of the liver. From the underside, the two additional lobes are located on the right lobe.[2] A line can be imagined running from the left of the vena cava and all the way forward to divide the liver and gallbladder into two halves.[3] This line is called Cantlie's line and is used to mark the division between the two lobes.[4] Other anatomical landmarks exist, such as the ligamentum venosum and the round ligament of the liver (ligamentum teres), which further divide the left side of the liver in two sections. An important anatomical landmark, the porta hepatis, also known as the transverse fissure of the liver, divides this left portion into four segments, which can be numbered in Roman numerals starting at the caudate lobe as I in an anticlockwise manner. From this parietal view, seven segments can be seen, because the eighth segment is only visible in the visceral view
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 7:05 pm عدل 1 مرات
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: liver segments السبت أبريل 13, 2024 7:51 pm
Segments
Liver segments Diagram showing the segments of the lobes as classified by Couinaud. The lobes of the liver are further divided into eight liver segments in the Couinaud system. These are also known as hepatic segments that are surgically resectable.[2]
Left lobe
The left lobe is smaller and more flattened than the right. It is situated in the epigastric, and left hypochondriacregions of the abdomen. Its upper surface is slightly convex and is moulded on to the diaphragm; its under surface presents the gastric impression and omental tuberosity.
Right lobe
The right lobe is six times the size of the left lobe. It occupies the right hypochondrium, on its posterior surface by the ligamentum venosum for the cranial (upper) half and by the ligamentum teres hepatis (Round ligament of liver) for the caudal (under) half. The ligamentum teres hepatis turns around the inferior margin of the liver to come out ventral in the falciform ligament. The right lobe is functionally separated from the left lobe by the middle hepatic vein. From a functional perspective (one that takes the arterial, portal venous, and systemic venous anatomy into account) the falciform ligament separates the medial and lateral segments of the left hepatic lobe.[6] The right lobe is of a somewhat quadrilateral form. Its under and posterior surfaces being marked by three fossæ: the fossa for the portal vein, the fossa for the gall-bladder and the fossae for the inferior vena cava. These separate the right lobe into two smaller lobes on its left posterior part: the quadrate lobe and the caudate lobe.
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 7:09 pm عدل 1 مرات
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
The quadrate lobe is an area of the liver situated on the undersurface of the medial segment left lobe (Couinaud segment IVb), bounded in front by the anterior margin of the liver, behind by the porta hepatis, on the right by the fossa for the gall-bladder, and on the left by the fossa for the umbilical vein. It is oblong in shape, its antero-posterior diameter being greater than its transverse.
Caudate lobe
The caudate lobe (posterior hepatic segment I) is situated upon the posterosuperior surface of the liver on the right lobe of the liver, opposite the tenth and eleventh thoracic vertebrae. The caudate lobe of the liver is bounded below by the porta hepatis, on the right by the fossa for the inferior vena cava, and on the left by the fossa for the ductus venosus and the physiological division of the liver, called the ligamentum venosum. It looks backward, being nearly vertical in position; it is longer from above downward than from side to side, and is somewhat concave in the transverse direction. It is situated behind the porta, and separates the fossa for the gall-bladder from the commencement of the fossa for the inferior vena cava. See Adriaan van den Spiegel 1578-1625 Spiegel's lobe. Budd–Chiari syndrome, caused by occlusion of hepatic venous outflow, can lead to hypertrophy of the caudate lobe due to its own caval anastomosis that allows for continued function of this lobe of the liver. The caudate lobe is named after the tail-shaped hepatic tissue (cauda; Latin, "tail") papillary process of the liver, which arise from its left side. It also has a caudate process (that is not tail-like shaped) arising from its right side, which provides surface continuity between the caudate lobe and the visceral surface of the anatomical right lobe of the liver.[2] The caudate process is a small elevation of the hepatic substance extending obliquely and laterally, from the lower extremity of the caudate lobe to the undersurface of the right lobe. The caudate lobe has a complex blood supply system. It derives its arterial supply from the caudate arteries, which arise from the right, left, and middle hepatic arteries that are connected to each other.[7] Besides, the caudate lobe also derives its supply from the right and left branches of the portal vein. Its venous drainage is through short hepatic veins that drain directly into the inferior vena cava (IVC) due to its proximity to the IVC
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 7:16 pm عدل 1 مرات
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Basic Sonographic Anatomy of the Liver السبت أبريل 13, 2024 8:00 pm
عدل سابقا من قبل د.كمال سيد في السبت مايو 11, 2024 7:16 pm عدل 1 مرات
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: LIVER ULTRASOUND السبت أبريل 13, 2024 8:03 pm
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: LIVER ULTRASOUND الإثنين أبريل 15, 2024 11:36 am
Mickey Mouse" view of Portal Triad It is a short axis, or "Mickey Mouse," view of the portal triad obtained as part of a biliary scan. Once the gallbladder is visualized in its long axis this view can be obtained by following the main lobar fissure, which has the appearance of a thin hyperechoic line extending from the neck of the gallbladder to the portal vein. The portal vein appears as the dot at the base "exclamation point" formed in this longitudinal view. With subtle fanning and adjustments of the probe, the remaining structures of the portal triad (the hepatic artery and common bile duct) can be brought into view. Given the smaller size of these structures they often have the appearance of Mickey Mouse ears. If the probe indicator is towards the patient's right side, then Mickey's right ear should be the common bile duct. Given the absence of flow in the common bile duct, doppler imaging can be helpful to differentiate it from the portal vein and hepatic artery. Once this view is obtained the probe can be rotated 90 degrees to obtain a long axis view of the CBD for measurement. Measurement should be taken from inner wall to inner wall of the CBD. Normal width of the CBD is 4 mm for patients less than 50 with one additional mm allowed for every decade over 40.
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Normal Liver Anatomy الأربعاء مايو 08, 2024 8:57 am
Normal Liver
Normal Anatomy
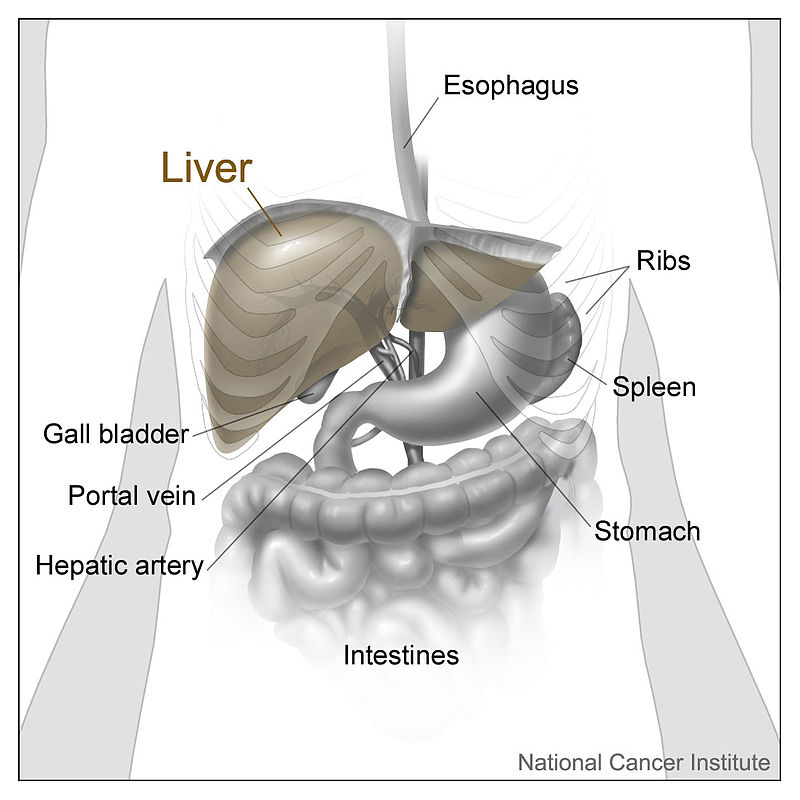
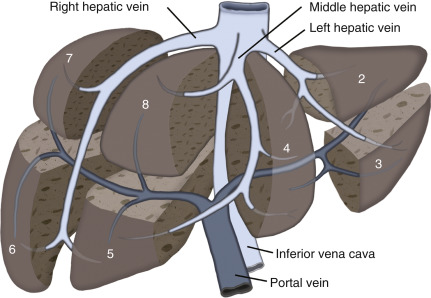
The 1/ cephalad portion of the liver is bounded by the diaphragm. 2/ The caudal extent of the liver is in close proximity to the stomach, the duodenum, and the large bowel and lies just cephalad to the pancreas. Using the 3/ Couinaud classification of liver anatomy, the liver is divided into eight segments. Segment 1 is the caudate lobe. The caudate’s boundary is the inferior vena cava (IVC) posteriorly and the portal vein and the echogenic fissure of the ligamentum venosum more anteriorly. The 4/ main lobar fissure, which extends from the gallbladder to the middle hepatic vein, divides the right from the left lobe of the liver ( Fig. 16.1 ). Knowledge of the location of the main lobar fissure is useful to locate the gallbladder, especially if the gallbladder is contracted or is full of stones. 5/ The gallbladder lies in the caudal extent of the main lobar fissure. 6/ The left lobe contains segments 2, 3, and 4A and 4B; the right lobe contains segments 5, 6, 7, and 8. 7/ The ligamentum teres is an easily identifiable landmark, which is the fibrous remnant of the umbilical vein. It separates segment 3 and segment 4B of the left lobe. The 8/ left hepatic vein can be thought of as the more cephalad extension of the ligamentum teres and divides segment 2 and segment 4A of the left lobe of the liver. The 9/right hepatic vein divides the more posterior segments 6/7 from the more anterior segments 5/8 of the right lobe ( Figs. 16.1 and 16.2 ).
Fig. 16.1 Segmental anatomy of the liver. The drawing shows a segmental anatomy of the liver with the middle hepatic vein dividing the right lobe of the liver (segments 5–8) from the left lobe of lobe liver (segments 2–4). The right hepatic vein divides segments 5 and 8 from segments 6 and 7, with a left hepatic vein dividing segments 2 and 3 from segment 4. Portal veins then divide the other segments of the liver.
From McGahan J. General and Vascular Ultrasound: Case Review . 3rd ed. Philadelphia, PA: Elsevier; 2016:294, Fig. S38-3.
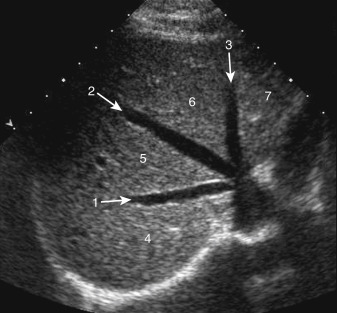
Fig. 16.2 Transverse image of the upper portion of the liver. ( 1 , right hepatic vein; 2 , middle hepatic vein; 3 , left hepatic vein. Segments of the liver include 4 , segment 7; 5 , segment 8; 6 , segment 4A; 7 , segment 2.)
From McGahan J. General and Vascular Ultrasound: Case Review . 3rd ed. Philadelphia, PA: Elsevier; 2016:279, Fig. S22-2.
The common hepatic artery (CHA) usually arises from the celiac artery and passes as the (PHA) proper hepatic artery anterior to the portal vein. Common hepatic artery variants include the right hepatic artery arising from the superior mesenteric artery and passing posterior to the portal vein as a replaced right hepatic artery. There are a number of variants of the origin and branches of the hepatic artery, including a replaced or accessory left hepatic artery. Most of these variants are not easily visualized with ultrasound (US). https://radiologykey.com/liver-and-spleen-3/
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: liver US Findings/Technique الأربعاء مايو 08, 2024 9:30 am
Ultrasound Findings/Technique
When scanning the liver, multiple transverse and longitudinal scans are obtained with the 1/ patient supine. Usually the liver is scanned with 2/ a curved array transducer with center frequency from 3 to 5 MHz. 3/Higher-frequency linear array transducers may be used to examine the liver surface to assess for cirrhotic nodules. The 4/ subcostal approach may be used for visualization of the right lobe, especially if the patient can hold a deep inspiration. Portions of the right lobe of the liver will require the patient to be placed in 5/ the right anterior oblique position. Using this technique, it is important to place the transducer parallel to the intercostal space. If this is not done, there will be acoustic shadowing from adjacent ribs, which prevents good visualization of the liver. The transducer often must be 6/ angled in a cephalad direction to scan the majority of the right lobe of the liver. Scanning performed 7/ intercostally may be helpful to identify the subdiaphragmatic portion of the liver, such as segments 7 and 8. Unfortunately, it may be difficult to visualize all portions of the right lobe of the liver because of the shadowing by the lung. This is why scanning in the intercostal space with the right side of the abdomen elevated is important. 8/ The left lobe can be scanned using an anterior subxiphoid approach. Normally, the liver 9/ appears as a A/ homogeneous structure, with B/ echogenicity slightly greater than or equal to the kidney. This internal comparison is important, as with increasing hepatic steatosis there will be increasing echogenicity of the liver. C/ The homogeneous echogenicity is only interrupted by the portal triads and the hepatic veins. 10/ The size of the liver is variable, with the length of the right lobe of the liver varying between 13 and 17 cm. Liver volume is not usually calculated, and there is considerable variability in the size of the right and left lobes of the liver. Color 11/ Doppler ultrasound is important to use to A/ identify the portal vein (PV) and its normal direction of hepatopetal flow (toward the liver). B/ In patients with cirrhosis, a) the portal vein can increase in size. Eventually there can be b) hepatofugal (reversed) flow in the portal vein. c) Color flow may be helpful to identify any thrombus in the portal vein. d) Pulsed Doppler ultrasound is used to identify the direction of flow in the portal vein. 12/ Color flow in the hepatic veins (HV) is easily obtained and is helpful to exclude occlusion of the hepatic veins. 13/ Pulse Doppler may be used to identify the normal triphasic hepatic waveform. The 14/ IVC can be identified posterior to the liver and heading anteriorly to the right atrium. The hepatic artery (HA) can be seen with color and noting its arterial waveform with pulsed Doppler. https://radiologykey.com/liver-and-spleen-3/
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: D/D RUQ cysts الأربعاء مايو 08, 2024 10:01 am
Liver: Etiologies of Right Upper Quadrant Pain
Hepatic Cysts
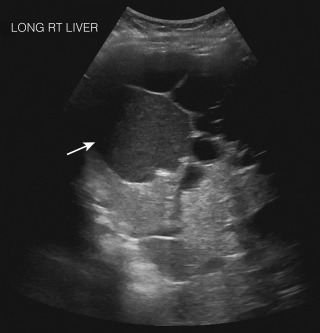
A hepatic cyst is rarely the etiology of right upper quadrant (RUQ) pain, unless it is large enough to distort the liver capsule or it has hemorrhaged internally. Cysts are 1/ A/ anechoic with B/ smooth walls with C/ good through transmission. 2/ Cysts with avascular septations or debris are called complex cysts . Upper abdominal pain may occur with hemorrhage into a hepatic cyst. 3/ Cysts with internal hemorrhage may become A/ echogenic, appear B/ more complex, or have C/ a fluid/blood interface ( Fig. 16.3 ). Although a complex cyst may be due to hemorrhage, the differential for a complex hepatic cyst is fairly broad ( Fig. 16.4 ). D/ The differential can include anything from a postoperative or posttransplant hematoma to postoperative seroma or biloma ( Fig. 16.5 ). Historical information is important in narrowing the ultrasound differential. Rarer causes of more complex hepatic cysts are listed in Table 16.1 . If a complex cyst is encountered, computed tomography (CT) or magnetic resonance imaging (MRI) may be useful for better characterization.
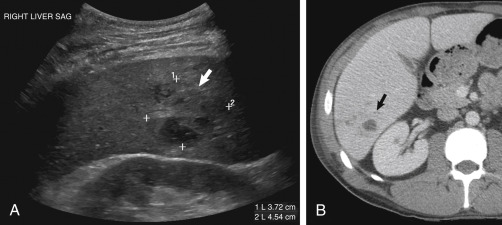
Fig. 16.3 Hemorrhagic cyst and polycystic liver disease. Ultrasound image through the liver 1/ demonstrates multiple small cysts within the liver, as well as 2/ a larger cyst with increased echoes ( arrow ) 3/ with good through transmission corresponding to a hemorrhagic cyst within the liver.
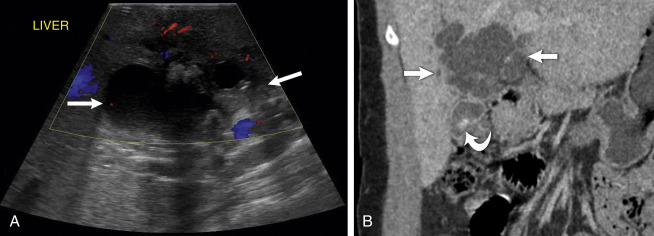
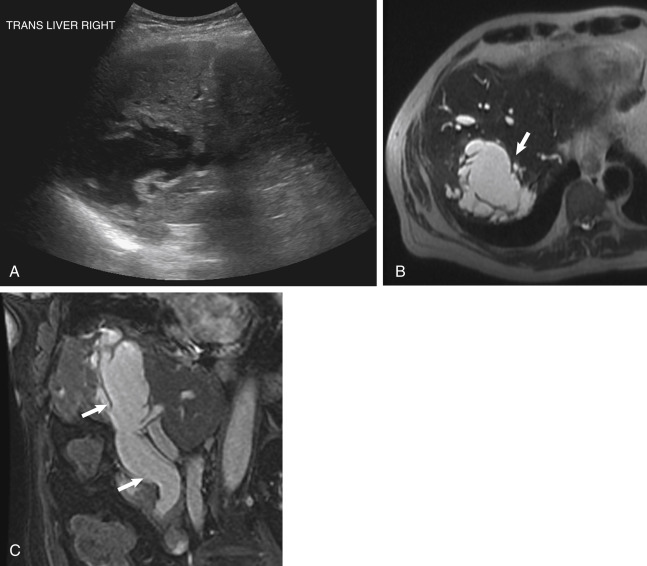
Fig. 16.4 Intrapapillary mucinous neoplasm of the liver. (A) Transverse ultrasound of the upper abdomen demonstrates a poorly marginated cyst with internal echoes. (B) Corresponding T2-weighted MRI demonstrates this multiseptated cyst ( arrow ). (C) This coronal T2-weighted MRI better demonstrates the communication between the multiseptated cyst and the common bile duct of this intrapapillary mucinous neoplasm ( arrows ) of the biliary tract.
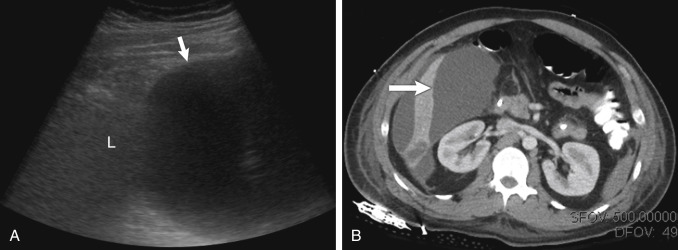
Fig. 16.5 Biloma. (A) Longitudinal scan of the liver ( L ) demonstrates a large fluid collection ( arrow ) in this postoperative patient with prior abdominal trauma. (B) Corresponding CT scan demonstrating large biloma ( arrow ). TABLE 16.1 Potential Differential of a Complex Hepatic Cyst
Hemorrhagic cyst
Pseudoaneurysms (use color flow)
Infected cyst
Polycystic renal disease (multiple hepatic cysts)
Biloma
Multiple hepatic cysts
Abscess
Mucinous (cystic) biliary tumor
Echinococcal cyst
Necrotic hepatic tumor
Abscess
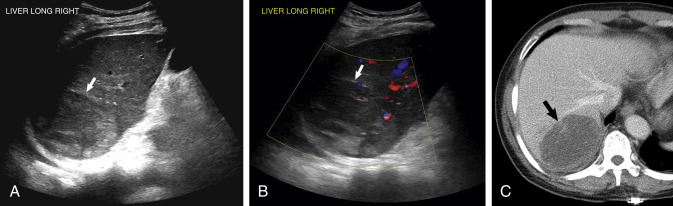
Bacterial liver abscesses are an etiology of acute abdominal pain. Bacterial abscesses are usually1/ hypoechoic but may be isoechoic or echogenic ( ). They may 2/ have thick or poorly defined walls ( Figs. 16.6 and 16.7 ). They may be difficult to diagnose on ultrasound. Therefore the clinical presentation is helpful. Again, CT or MRI may be needed to better characterize an hepatic abscess. 3/ Liver abscesses may be secondary to infection from adjacent structures, such gallbladder perforation into the liver from acute cholecystitis ( Fig. 16.8 , ). An hepatic 4/ abscess may also occur from hematogenous spread due to acute diverticulitis or appendicitis. It is important to realize that although abscesses often appear complex with thick internal separations, they may also appear 5/ solid and could be confused with a solid mass (see Figs. 16.6 and 16.7 ). Fig. 16.6 Liver abscess: K. pneumoniae. (A) Transverse ultrasound of the upper abdomen demonstrates an isoechoic or slightly hypoechoic mass ( arrow ) in the right lobe of the liver, which represented a bacterial liver abscess. (Note small right pleural effusion). (B) Color Doppler ultrasound demonstrates very little color flow noted within this abscess ( arrow ). (C) CT scan with contrast of the upper abdomen demonstrates a well-demarcated, low-density mass ( arrow ), which was later drained percutaneously with the specimen cultured that revealed an abscess due to K. pneumoniae .
Fig. 16.7 Echogenic bacterial liver abscess. (A) Longitudinal ultrasound demonstrated a primarily echogenic mass ( calipers and arrow ). There is a small cystic component noted posteriorly. (B) Contrast-enhanced CT scan demonstrated the majority of the abscess ( arrow ) was not easily identified except for the cystic component of the mass. Fig. 16.8 Liver abscess secondary to perforated gallbladder. (A) Transverse ultrasound through the caudal aspect of the right lobe of the liver demonstrates thick-walled, poorly demarcated fluid collection ( arrows ), which corresponded to a liver abscess from a perforated gallbladder. (B) Coronal CT scan demonstrates the liver abscess ( arrows ) and part of the gallbladder with a radiopaque stone ( curved arrow ). https://radiologykey.com/liver-and-spleen-3/








 الجمعة فبراير 08, 2013 9:24 pm
الجمعة فبراير 08, 2013 9:24 pm

 The
The 
 ). They may 2/ have thick or poorly defined walls ( Figs. 16.6 and 16.7 ). They may be difficult to diagnose on ultrasound. Therefore the clinical presentation is helpful. Again, CT or MRI may be needed to better characterize an hepatic abscess. 3/ Liver abscesses may be secondary to infection from adjacent structures, such gallbladder perforation into the liver from acute cholecystitis ( Fig. 16.8 ,
). They may 2/ have thick or poorly defined walls ( Figs. 16.6 and 16.7 ). They may be difficult to diagnose on ultrasound. Therefore the clinical presentation is helpful. Again, CT or MRI may be needed to better characterize an hepatic abscess. 3/ Liver abscesses may be secondary to infection from adjacent structures, such gallbladder perforation into the liver from acute cholecystitis ( Fig. 16.8 ,