عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Vascular US & Doppler الإثنين فبراير 11, 2013 5:46 am
Aorta Ultrasound - Introduction - SonoSite, Inc.
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Aortic Aneurysms الثلاثاء مايو 07, 2024 7:42 am
Duplex assessment of aneurysms and endovascular repair True aneurysms are abnormal dilations of arteries. The term ectasia is often used to describe a moderate dilation of arteries. The abdominal aorta is one of the commonest sites for aneurysms to occur. The main risk of abdominal aortic aneurysms (AAA) is rupture, which is fatal in most cases. In the USA rupture of an AAA is the 14th commonest cause of death and is estimated to kill approximately 10 000 people per year (Birkmeyer & Upchurch 2007). In England and Wales, this figure is approximately 5000 people (Office for National Statistics 2006). Men over the age of 65 years are the most common group to be affected. Ultrasound can detect almost all AAAs and, when screening is combined with elective surgery, the mortality associated with the disease is almost halved (Ashton et al. 2002). A recent analysis of four large, randomized clinical trials has also confirmed that population-based screening substantially reduces AAA-related mortality in selected patient groups (Fleming et al. 2005) In the USA, the US Preventive Services Task Force (2005) and a consortium of leading professional organizations recommend one-time screening with abdominal ultrasonography for all men aged 65–75 years who have ever smoked. In the UK, a national screening program should be under way by the time this edition is published. Ultrasound is the obvious modality for screening as it is a rapid, cheap, and simple noninvasive method of detecting aneurysms and can be used for serial investigations to monitor any increase in size of small aneurysms. However, if surgical intervention is being considered, other imaging techniques, such as computed tomography (CT) and magnetic resonance imaging (MRI), are required to demonstrate the relationship of an aneurysm to major branches and other structures within the body. In the past, treatment of AAA was by open surgery but nowadays approximately 50% of patients are treated by the less invasive technique of endovascular aortic aneurysm repair (EVAR), where a stent graft is inserted via the femoral arteries. Endovascular repair can also be used to treat aneurysms in other areas of the body. This chapter concentrates on ultrasound scanning of aortic aneurysms and surveillance of EVAR procedures but also considers the assessment of aneurysms in other areas of the peripheral circulation.
Definition of an aneurysm
It has been suggested that an aneurysm is a 1/ permanent 2/ localized 3/ dilation of an artery having at least a 4/ 50% increase in diameter compared to the normal expected diameter (Johnston et al. 1991). Ectasia is characterized by a diameter increase <50% of the normal expected diameter. It is worth remembering that there is considerable variability in the normal diameter of arteries among individuals, and this will be dependent on factors such as physical size, sex, and age. ANATOMY OF THE ABDOMINAL AORTA
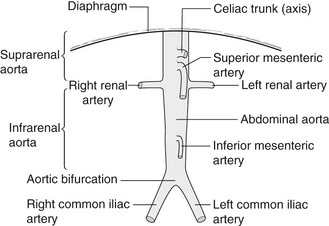
The abdominal aorta 1/ commences at the level of the diaphragm and lies 2/ just in front of the spine. It descends3/ slightly to the left of the midline to the level of the fourth lumbar vertebra, 4/ where it divides into the left and right common iliac arteries (Fig. 11.1). 5/ It tapers slightly as it descends, owing to the large branches it gives off. 6/ Major branches of the aorta that can be easily identified with ultrasound include the celiac axis and superior mesenteric artery (SMA) (Fig. 11.2). These can act as important reference points when determining the upper limit of an aneurysm. Visualization of the inferior mesenteric artery is variable. The 7/ vena cava lies to the right of the aorta and may assume a variety of shapes, especially in the presence of an aneurysm, and commonly appears ‘flattened’ when compared to the circular shape of the aorta. Figure 11.1 Anatomy of the abdominal aorta and its major branches.
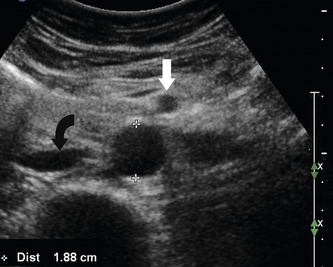
Figure 11.2 A transverse image of a normal abdominal aorta. The inferior vena cava (curved arrow) is seen to the right of the aorta and the superior mesenteric artery (straight arrow) is seen anterior to the aorta (note that the probe orientation means that the right side of the patient is on the left of the image).
PATHOLOGY OF ANEURYSMS
The mechanism of aneurysm development is uncertain but may involve a multifactorial process leading to the destruction of aortic wall connective tissue. There is evidence that increased local production of enzymes capable of degrading elastic fibers as well as interstitial collagens is associated with AAA (Wassef et al. 2001). The lumen of an aneurysm is often lined with large amounts of thrombus that can be a potential source of emboli. This is also why arteriograms, which only demonstrate the flow lumen, are not accurate for estimating the true diameter of an aneurysm, as the flow lumen can be significantly smaller than the diameter of the entire vessel. Aortic aneurysms can also extend into the iliac arteries. Some aortic aneurysms are involved in an inflammatory process, with marked periaortic fibrosis surrounding the aorta making surgical resection difficult (see Figure 11.12D). Aneurysms can also be caused by a variety of infections, such as bacterial endocarditis, and are termed mycotic aneurysms. These can occur anywhere in the body. Popliteal aneurysms may be the source of distal emboli. They can also occlude, leading to symptoms of acute lower-limb ischemia. This should always be considered as a potential cause of the acutely ischemic leg, especially in patients with no other obvious risk factors.
False aneurysms occur predominantly in the femoral artery following puncture of the arterial wall for catheter access. In this situation, blood continues to flow backward and forward through the puncture site into a false flow cavity outside the artery.
ANEURYSM SHAPES AND TYPES
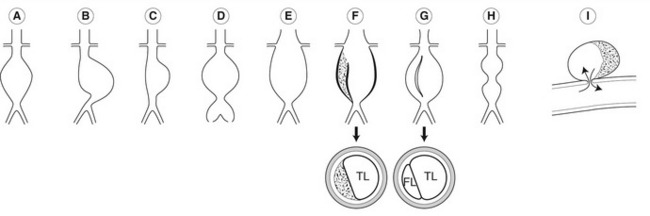
Aneurysms vary considerably in shape and size (Fig. 11.3). Most aneurysms are fusiform in shape and there is uniform dilation across the entire cross-section of the vessel. Saccular aneurysms exhibit a typical localized bulging of the wall. Dissecting aneurysms occur due to a disruption of the intimal lining of the vessel, allowing blood to enter the subintimal space. This can result in the stripping of the intima, and sometimes of the media, from the artery wall. If the aorta partially dissects, large amounts of thrombus may be seen in the subintimal space (Fig. 11.3F). If there is a full dissection, a false flow lumen is created and the dissected layer of intima may be seen flapping freely in time with arterial pulsation (Fig. 11.3G). Some aortic dissections are not associated with aneurysms and can start in the chest, extending through the aorta into the iliac arteries. It is possible for aortic branches, such as renal arteries, to be supplied via either lumen. Occasionally, two aneurysmal dilations may be seen along the length of the abdominal aorta, separated by a normal segment of the aorta, which gives rise to a classic “dumb-bell” shape when viewed in longitudinal section (Fig. 11.3H). As the aorta dilates, it also tends to increase in length, producing tortuosity that often shifts the aorta to the left of the midline or deflects it in an anterior direction. Figure 11.3 Aneurysms are very variable in shape and type. (A) Fusiform infrarenal aortic aneurysm. (B) Tortuous elongated aortic aneurysm with the sac shifted to the left of the midline. (C) Saccular aortic aneurysm. (D) Infrarenal aortic aneurysm extending into the iliac arteries. (E) Suprarenal aortic aneurysm involving the renal arteries. (F) Dissecting aortic aneurysm with a tear between the intima and media allowing blood into the subintimal space. (G) Dissecting aortic aneurysm in which the intima has fully dissected, creating a false flow lumen. (H) Double aneurysm of the aorta producing a “dumb-bell” appearance. (I) False aneurysm of the common femoral artery following arterial puncture. TL, true lumen; FL, false lumen. https://radiologykey.com/duplex-assessment-of-aneurysms-and-endovascular-repair/
عدل سابقا من قبل د.كمال سيد في الثلاثاء مايو 07, 2024 7:59 am عدل 1 مرات
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Aortic Aneurysms الثلاثاء مايو 07, 2024 7:57 am
AORTIC ANEURYSMS: SYMPTOMS AND TREATMENT
The normal size of the abdominal aorta varies between 1.4 and 2.5 cm in diameter (Johnston et al. 1991) (Fig. 11.2). An aortic diameter slightly above 2.5 cm is considered mildly abnormal or ectatic. A small aortic aneurysm is generally regarded as an aorta having a diameter of 3 cm, and many surgeons will not request serial screening scans unless the aorta reaches this level. However, some vascular units monitor patients with slightly enlarged aortas, especially if the patient is young (<55 years old). As the aorta increases in size, there is a potential for rupture due to increased tension in the arterial wall. The UK Small Aneurysm Trial Participants (1998) demonstrated that the average annual growth rate of aneurysms measuring between 4 and 5.5 cm was 0.33 cm a year. However, rates will vary among individuals and are also dependent on the size of the aneurysm. The prevalence of aortic aneurysms is five to six times greater in men than women (Vardulaki et al. 2000). In addition, there seems to be a strong familial link, with siblings of aneurysm patients having a higher risk of developing an aneurysm compared with the general population. Clinically, there are usually no symptoms associated with the development of an aortic aneurysm and many are discovered incidentally, during routine examinations or on plain abdominal radiographs. Occasionally, patients present with symptoms of renal hydronephrosis. This is caused by compression of a ureter leading from one of the kidneys by the aneurysm sac and most frequently occurs on the left side. The symptoms associated with aneurysm leakage or rupture include back or abdominal pain and acute shock. Ultrasound is occasionally used to confirm the diagnosis in the emergency room, although the symptoms are usually so acute that emergency surgery is required. However an emergency room scan that excludes an aneurysm can be useful and many emergency physicians have been trained to undertake rapid AAA scanning. The mortality rate for acute rupture of an aortic aneurysm is very high, 65–85% (Kniemeyer et al. 2000), and many patients do not reach hospital alive. The risk of aortic aneurysm rupture increases with size. The UK Small Aneurysm Trial Participants (1998) found that the mean risk of rupture of aneurysms measuring 4–5.5 cm was 1% per year. However, larger aneurysms carry a higher rate of rupture. A study by Lederle et al. (2002) demonstrated that the average risk of rupture in male patients with a 6−6.9 cm aneurysm was 10% per year and 32% per year for aneurysms measuring more than 7 cm in diameter. Clearly, there are benefits in detecting aneurysms at an early stage so that serial follow-up can be carried out and elective repair performed if the aneurysm becomes too large. The UK Small Aneurysm Trial Participants (1998) have shown no survival benefit for open repair of aneurysms measuring less than 5.5 cm in diameter compared to ultrasound surveillance and this was also confirmed after a 12-year follow-up analysis of the trial (The UK Small Aneurysm Trial Participants 2007). In the original study, age, sex, or initial aneurysm size did not modify the overall hazard ratio. Therefore, many surgeons will only carry out elective repair if the aneurysm has a diameter of equal to or greater than 5.5 cm, or if there are indications that smaller aneurysms are becoming symptomatic and are at risk of rupturing. Although aortic aneurysms are much more prevalent in men, there is some evidence that women with aneurysms in the 5–5.9 cm range may be up to four times more likely to undergo rupture compared to men with similar-sized aneurysms (Brown et al. 2003). Further research may prompt a lower threshold for repairing aneurysms in female patients. However, at the present time the mass screening of women does not appear to be cost-effective. PRACTICAL CONSIDERATIONS FOR DUPLEX SCANNING OF AORTIC ANEURYSMS
What information does the physician require?
• The maximum diameter of the aorta
• Any relevant aneurysm features such as shape or position
• Does the aneurysm extend across the iliac bifurcation into the common iliac arteries?
• Indications of thrombus load or mobile areas of thrombus
It is important to note any limitations of the scan and to state clearly what measurements were made and from what positions. Situations have occurred in which the points of measurement have been ambiguously reported and the overall length of an aneurysm has been mistakenly interpreted as its diameter.
The purpose of the scan is to determine if there is an aneurysm involving the aorta or peripheral arterial system and, if appropriate, to monitor the size of the aneurysm on a serial basis. A screening scan can be performed in less than 5 min, but more detailed scans of endovascular grafts may take up to 20 min. https://radiologykey.com/duplex-assessment-of-aneurysms-and-endovascular-repair/
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Blood flow and its appearance on color flow imaging الثلاثاء مايو 07, 2024 8:31 am
Blood flow and its appearance on color flow imaging Arterial blood flow is complex and consists of pulsatile flow of an inhomogeneous fluid through viscoelastic arteries that branch, curve, and taper. However, a useful understanding of hemodynamics can be gained by first considering simple models, such as steady flow in a rigid tube. Factors affecting venous flow will also be considered. This will allow us to interpret spectral Doppler and color Doppler images of blood flow more easily. However, when interpreting color flow images it is important to remember that the color represents the mean velocity of flow obtained from the sample volumes and that this will depend on the angle between the ultrasound beam and blood flow. The pulse repetition frequency (PRF) and filter setting used and the length of time over which the image is created may also affect the appearance of the image. Artifactual effects also have to be considered carefully before drawing conclusions about the blood flow. STRUCTURE OF VESSEL WALLS The arterial and venous systems are often thought of as a series of tubes that transport blood to and from organs and tissues. In reality, blood vessels are highly complex structures that respond to nervous stimulation and interact with chemicals in the blood stream to regulate the flow of blood throughout the body. Changes in cardiac output and the tone of the smooth-muscle cells in the arterial walls are crucial factors that affect blood flow. The structure of a blood vessel wall varies considerably depending on its position within the vascular system. Arteries and veins are composed of three layers of tissue, with veins having thinner walls than arteries. The 1/ outer layer is called the adventitia and is predominantly composed of A/ connective tissue B/ with collagen and C/ elastin. The 2/ middle layer, the media, is the thickest layer and is composed of smooth-muscle fibers and elastic tissue. The 3/ intima is the inner layer and consists of a thin layer of endothelium overlying an elastic membrane. The capillaries, by contrast, consist of a single layer of endothelium, which allows for the exchange of molecules through the capillary wall. It is possible to image the structure of larger vessel walls using ultrasound and to identify the early stages of arterial disease, such as intimal thickening. The arterial tree consistsof 1/ elastic arteries, 2/ muscular arteries, 3/ and arterioles. The aorta and subclavian arteries are examples of elastic or conducting arteries and contain elastic fibers and a large amount of collagen fibers to limit the degree of stretch. Elastic arteries function as a pressure reservoir, as the elastic tissue in the vessel wall is able to absorb a proportion of the large amount of energy generated by the heart during systole. This maintains the end-diastolic pressure and decreases the load on the left side of the heart. Muscular or distributing arteries, such as the radial artery, contain a large proportion of smooth-muscle cells in the media. These arteries are innervated by nerves and can dilate or constrict. The muscular arteries are responsible for regional distribution of blood flow. Arterioles are the smallest arteries, and their media is composed almost entirely of smooth-muscle cells. Arterioles have an important role in controlling blood pressure and flow, and they can constrict or dilate after sympathetic nerve or chemical stimulation. The arterioles distribute blood to specific capillary beds and can dilate or constrict selectively around the body depending on the requirements of organs or tissues. WHY DOES BLOOD FLOW? Energy created by the contraction of the heart forces blood around the body. Blood flow in the arteries depends on two factors: (1) the energy available to drive the blood flow, and (2) the resistance to flow presented by the vascular system. A scientist named Daniel Bernoulli (1700–1782) showed that the total fluid energy, which gives rise to the flow, is made up of three parts: • Pressure energy (p) – this is the pressure in the fluid, which, in the case of blood flow, varies due to the contraction of the heart and the distension of the aorta. • Kinetic energy (KE) – this is due to the fact that the fluid is a moving mass. Kinetic energy is dependent on the density (ρ) and velocity (V) of the fluid:
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Why does blood flow ? الثلاثاء مايو 07, 2024 8:36 am
(5.1)
• Gravitational potential energy – this is the ability of a volume of blood to do work due to the effect of gravity (g) on the column of fluid with density (ρ) because of its height (h) above a reference point, typically the heart. Gravitational potential energy (ρgh) is equivalent to hydrostatic pressure but has an opposite sign (i.e.−ρgh). For example, when a person is standing, there is a column of blood – the height of the heart above the feet – resting on the blood in the vessels in the foot (Fig. 5.1A) causing a higher pressure, due to the hydrostatic pressure, than that seen when the person is lying down (Fig. 5.1B). As the heart is taken as the reference point, and the feet are below the heart, the hydrostatic pressure is positive. If the arm is raised so that it is above the heart, the hydrostatic pressure is negative, causing the veins to collapse and the pressure in the arteries in the arm to be lower than the pressure at the level of the heart. The total fluid energy is given by: Figure 5.1 Schematic diagram showing typical pressures in arteries and veins with the subject standing (A) and lying (B). The component due to hydrostatic pressure when the subject is vertical is shown alongside A. (5.2) Figure 5.2 gives a graphical display of how the total energy, kinetic energy, and pressure alter with continuous flow through an idealized narrowing. Usually the kinetic energy component of the total energy is small compared with the pressure energy. When fluid flows through a tube with a narrowing, the fluid travels faster as it passes through the narrowed section. As the velocity of the fluid increases in a narrowed portion of the vessel, the kinetic energy increases and the potential energy (i.e., the pressure) falls. The pressure within the narrowing is therefore lower than the pressure in the portion of the vessel before the narrowing. As the fluid passes beyond the narrowing, the velocity drops again and the kinetic energy is converted back to potential energy (the pressure), which increases. Energy is lost as the fluid passes through the narrowing (Fig. 5.2), with the extent of the entrance and exit losses depending on the geometry and degree of the narrowing (Oates 2008). In normal arteries, very little energy is lost as the blood flows away from the heart toward the limbs and organs, and the mean pressure in the small distal vessels is only slightly lower than in the aorta. However, in the presence of significant arterial disease, energy may be lost from the blood as it passes through tight narrowings or small collateral vessels around occlusions, leading to a drop in the pressure greater than that which would be expected in a normal artery; this can lead to reduced blood flow and tissue perfusion distally. Because the entrance and exit losses account for a large proportion of the pressure loss, it is likely that two adjacent stenoses will have a more significant effect than one long one (Oates 2008). Figure 5.2 Diagram showing how energy losses can occur across a narrowing. KE, kinetic energy. RESISTANCE TO FLOW In 1840, a physician named Poiseuille established a relationship between flow, the pressure gradient along a tube, and the dimensions of a tube. The relationship can simply be understood as: (5.3) where the resistance to flow is given by: (5.4) where r is the radius. Viscosity causes friction between the moving layers of the fluid. Treacle, for example, is a highly viscous fluid, whereas water has a low viscosity and therefore offers less resistance to flow when traveling through a small tube.
د.كمال سيد Admin
عدد المساهمات : 2690نقاط : 4494السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Vascular US & Doppler الثلاثاء مايو 07, 2024 8:40 am
Poiseuille’s law shows that the resistance to flow is highly dependent on changes in the radius (r4). In the normal circulation, the greatest proportion of the resistance is thought to occur at the arteriole level. Tissue perfusion is controlled by changes in the diameter of the arterioles. The presence of arterial disease in the arteries, such as stenoses or occlusions, can significantly alter the resistance to flow, with the reduction in vessel diameter having a major effect on the change in resistance seen. In severe disease, the arterioles distal to the disease may become maximally dilated in order to reduce the peripheral resistance, thus increasing blood flow in an attempt to maintain tissue perfusion. Poiseuille described nonpulsatile flow in a rigid tube, so his equation does not completely represent arterial blood flow; however, it gives us some understanding of the relationship between pressure drop, resistance, and flow.
VELOCITY CHANGES WITHIN STENOSES
We have already seen that fluid travels faster through a narrowed section of tube. The theory to determine these changes in velocity is described below. The volume flow through the tube is given by:
(5.5)
where V is the mean velocity across the whole of the vessel, averaged over time, and A is the cross-sectional area of the tube. If the tube has no outlets or branches through which fluid can be lost, the flow along the tube remains constant. Therefore, the velocity at any point along the tube depends on the cross-sectional area of the tube. Figure 5.3 shows a tube of changing cross-sectional area (A1, A2); now, as the flow (Q) along the tube is constant: Figure 5.3 Change in cross-sectional area. As the flow is constant through the tube, the velocity of the fluid increases from V1 to V2 as the cross-sectional area decreases from A1 to A2.
(5.6)
This equation can be rearranged to show that the change in the velocities is related to the change in the cross-sectional area, as follows:
(5.7)
As the cross-sectional area depends on the radius r of the tube (A = πr2), we have:
(5.
This relationship describes steady flow in a rigid tube, but it does give us an indication as to how the velocity will change across a stenosis in an artery.
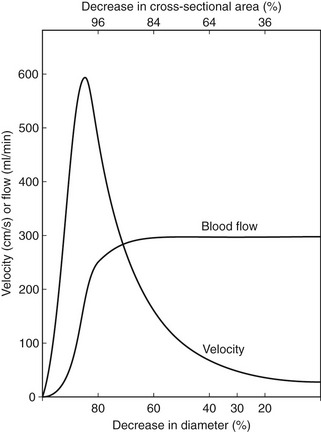
Figure 5.4 shows how the flow and velocity within an idealized stenosis vary with the degree of diameter reduction caused by the stenosis, based on the predictions from a simplified theoretical model. On the right-hand side of the graph, where the diameter reduction is less than 70–80%, the flow remains relatively unchanged as the diameter of the vessel is reduced. This is because the proportion of the resistance to flow due to the stenosis is small compared with the overall resistance of the vascular bed that the vessel is supplying. However, as the diameter reduces farther, the resistance offered by the stenosis becomes a significant proportion of the total resistance, and the stenosis begins to limit the flow. This is known as a hemodynamically significant stenosis. At this point, the flow decreases quickly as the diameter is reduced. Figure 5.4 Changes in flow and velocity as the degree of stenosis alters, predicted by a simple theoretical model of a smooth, symmetrical stenosis.
(Spencer & Reid, Quantitation of carotid stenosis with continuous-wave (C-W), Doppler Ultrasound. Stroke 10:326-330, 1979)
The graph also predicts the behavior of the velocity as the vessel diameter is reduced and shows that the velocity increases with diameter reduction. Noticeable changes in velocity begin to occur at much smaller diameter reductions than would produce a flow reduction. Therefore, measurement of velocity changes is a more sensitive method of detecting small-vessel lumen reductions than measurement of flow. Measurements of velocity made using Doppler ultrasound are also more accurate than measurement of flow, as will be discussed later (see Ch. 6). Therefore, it is usually the change in velocity of blood within a diseased artery that is used to quantify the degree of narrowing. Eventually, there comes a point at which the resistance to flow produced by the narrowing is so great that the flow drops to such an extent that the velocity begins to decrease, as shown on the left side of the graph. This is seen as ‘trickle flow’ within the vessel. It is especially important to be able to identify trickle flow within a stenosis as the peak velocities seen may be similar to those seen in healthy vessels, but the color image and waveform shapes will not appear normal. As blood flow is pulsatile and arteries are nonrigid vessels, it is difficult to predict theoretically the velocity increase that would be seen for a particular diameter reduction. Instead, velocity criteria used to quantify the degree of narrowing are produced by comparing Doppler velocity measurements with arteriogram results, as arteriography has been considered to be the ‘gold standard’ for the diagnosis of arterial disease. https://radiologykey.com/blood-flow-and-its-appearance-on-color-flow-imaging/








 الإثنين فبراير 11, 2013 5:46 am
الإثنين فبراير 11, 2013 5:46 am
 (5.1)
(5.1)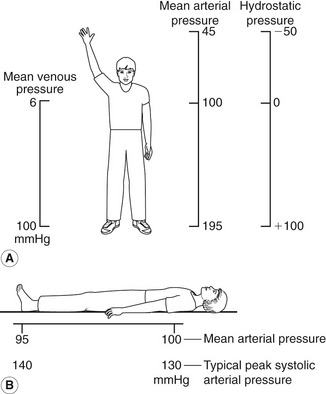
 (5.2)
(5.2)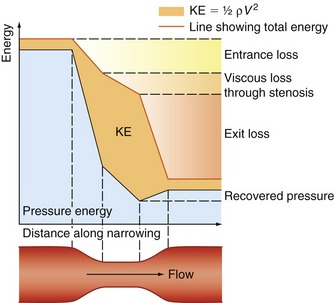
 (5.3)
(5.3) (5.4)
(5.4)
 (5.5)
(5.5)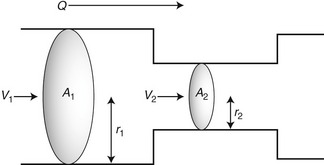
 (5.6)
(5.6) (5.7)
(5.7) (5.
(5.