عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Pyloric Stenosis الأربعاء أبريل 17, 2024 8:13 pm
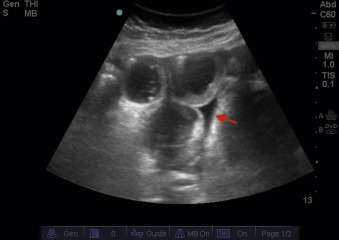
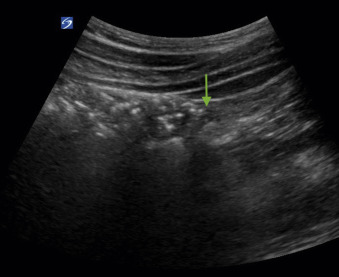
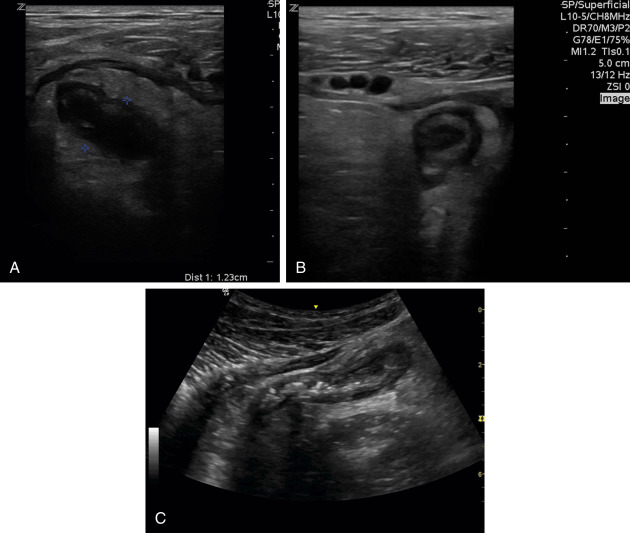
Pyloric Stenosis (Infant with Vomiting) Like many pathologies in pediatrics, pyloric stenosis is best evaluated with ultrasound. Remember, pyloric stenosis is caused by 1/hypertrophy of the muscular layer of the pylorus and 2/ failure of the pylorus to relax, leading to 3/ gastric outlet obstruction. Pyloricstenosis is the most common cause of vomiting requiring surgery in infants. It is more common in first born male infants. To locate the pylorus on ultrasound, use the linear probe in a transverse position and first locate the gallbladder. The pylorus should be found posterior to the gallbladder. If the pylorus is thickened, you can see a “target” or “donut” sign To assess for pyloric stenosis, first measure the muscular layer of pylorus in longitudinal and transverse views. >3mm thickness raises concern for hypertrophy. Then measure the length of the pyloric canal. There is a range in the radiology literature for abnormal pyloric channel length from >15 to 19 mm Another way to evaluate the pylorus is to check for passage of gastric contents : if you see gastric contents moving freely through an open pylorus, then pyloric stenosis is much less likely
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 17, 2024 8:16 pm
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 17, 2024 8:17 pm
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 17, 2024 8:18 pm
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 17, 2024 8:24 pm
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 17, 2024 8:31 pm
Pyloric stenosis is an uncommon condition in infants that blocks food from entering the small intestine. Typically, a muscular valve between the stomach and small intestine holds food in the stomach until it is ready for the next stage in the digestive process. This valve is called the pylorus valve. In pyloric stenosis, the pylorus muscles thicken and become abnormally large, blocking food from reaching the small intestine.
Pyloric stenosis can lead to forceful vomiting, dehydration and weight loss. Babies with pyloric stenosis may seem to be hungry all the time. Surgery cures pyloric stenosis. Symptoms of pyloric stenosis usually appear within 3 to 5 weeks after birth. Pyloric stenosis is rare in babies older than 3 months. Symptoms include:
Vomiting after feeding. The baby may vomit forcefully, ejecting breast milk or formula up to several feet away. This is known as projectile vomiting. Vomiting might be mild at first. But over time, it becomes more severe as the pylorus opening narrows. The vomit may sometimes contain blood.
Persistent hunger. Babies who have pyloric stenosis often want to eat soon after vomiting.
Stomach contractions. You may notice wavelike contractions that ripple across your baby's upper stomach area soon after feeding but before vomiting. These contractions are part of the digestive process known as peristalsis. The contractions are caused by stomach muscles trying to force food through the narrowed pylorus.
Dehydration. Your baby might cry without tears or become lethargic. You might find yourself changing fewer wet diapers or diapers that aren't as wet as you expect.
Changes in bowel movements. Since pyloric stenosis prevents food from reaching the intestines, babies with this condition might be constipated.
Weight problems. Pyloric stenosis can keep a baby from gaining weight, and sometimes can cause weight loss.
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 17, 2024 8:34 pm
See your baby's doctor if your baby:
Projectile vomits after feeding.
Seems less active or unusually irritable.
Urinates much less frequently or has noticeably fewer bowel movements.
Isn't gaining weight or is losing weight.
Causes
The causes of pyloric stenosis are unknown, but genetic and environmental factors might play a role. Pyloric stenosis usually isn't present at birth and probably develops afterward.
Risk factors
Risk factors for pyloric stenosis include:
Sex. Pyloric stenosis is seen more often in boys, especially firstborn children, than in girls.
Race and ethnicity. Pyloric stenosis is more common in white and Hispanic children.
Premature birth. Pyloric stenosis is more common in babies born prematurely than in full-term babies.
Family history. Studies found higher rates of this disorder among certain families. Pyloric stenosis develops in about 20% of male descendants and 10% of female descendants of mothers who had the condition.
Smoking during pregnancy. This behavior can nearly double the risk of pyloric stenosis.
Early antibiotic use. Babies given certain antibiotics in the first weeks of life — erythromycin to treat whooping cough, for example — have an increased risk of pyloric stenosis. In addition, babies born to mothers who took certain antibiotics in late pregnancy may have an increased risk of pyloric stenosis.
Bottle-feeding. Some studies suggest that bottle-feeding rather than breastfeeding can increase the risk of pyloric stenosis. Most of the people who participated in these studies used formula rather than breast milk, so it isn't clear whether the increased risk is related to formula or the mechanism of bottle-feeding.
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 17, 2024 8:36 pm
Complications
Pyloric stenosis can lead to:
Failure to grow and develop.
Dehydration. Frequent vomiting can cause dehydration and a mineral imbalance. These minerals are called electrolytes. Electrolytes help regulate many vital functions.
Stomach irritation. Repeated vomiting can irritate your baby's stomach and may cause mild bleeding.
Jaundice. Rarely, a substance secreted by the liver can build up, causing a yellowing of the skin and eyes. This substance is known as bilirubin.
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: US Abdomen Complete Protocol الأحد أبريل 21, 2024 12:25 pm
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 24, 2024 5:20 pm
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: Abdominal Ultrasound الأربعاء أبريل 24, 2024 5:22 pm
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Lower Abdomen and Bowel الأربعاء مايو 08, 2024 7:48 pm
Lower Abdomen and Bowel
Bowel Ultrasound
Normal Anatomy
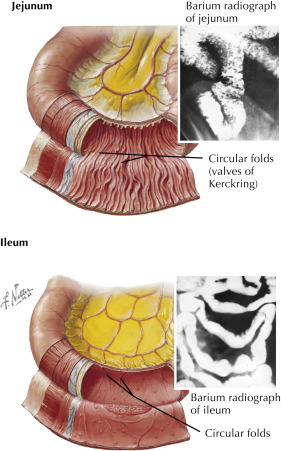
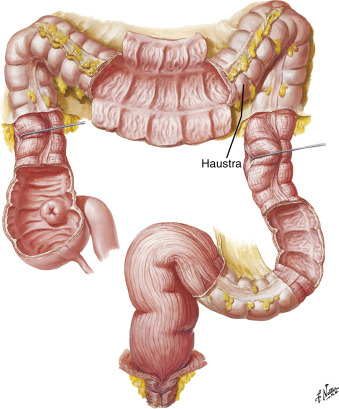
The small bowel consists 1/ of the bowel (distal to the stomach and proximal to the colon). 2/ It is approximately 5 meters long and includes 3/ the duodenum, jejunum, and ileum. 4/ The small bowel contains prominent mucosal folds known as (plicae circularesORvalvular connvinetes).5/ The jejunum has the most developed and highest concentration of these folds, which remain present even in distended bowel ( Fig. 21.1 ). The 6/ plicae circulares (circular folds {valves of Kerckring}) decrease in density as you move distally to a nearly smooth distal ileum. 7/ The mucosal layer of small bowel contains finger-like projections into the lumen called villi . Fig. 21.1 Normal small bowel containing plicae circulares (circular folds), also called valves of Kerckring . The jejunum has the highest concentration of these mucosal folds, which decrease in density in the ileum. Reprinted from Netter Anatomy Illustration Collection. Elsevier Inc. All Rights Reserved. The large bowel1/ begins with the cecum and includes the entire colon and rectum ( Fig. 21.2 ). 2/ At the point where the ileum joins the cecum, a sphincter is present (ileocecal valve) that prevents the backflow of contents into the small bowel. 3/ The cecum is a pouchlike structure that usually contains gas. 4/ The large bowel does NOT contain villi, and there are NO major mucosal folds (excluding the rectum).5/ The wall of the colon is creased by its muscular layer, including its serosa, into small sacs called haustra . This gives the colon a segmented appearance.
Fig. 21.2 The large bowel contains haustra, which are folds in the wall that create its segmented appearance. Reprinted from Netter Anatomy Illustration Collection. Elsevier Inc. All Rights Reserved.
Ultrasound Techniques and Normal Findings
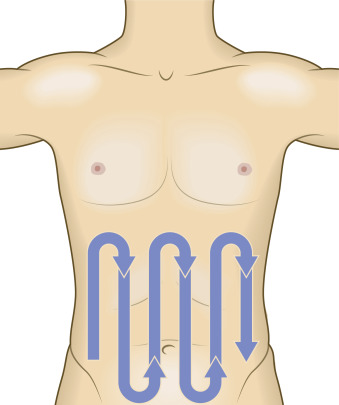
Imaging of the bowels is performed 1/ using a low-frequency transducer, such as a curvilinear probe (typically 3- to 6-MHz frequency), which allows for A/ good penetration and B/ a large field of view. The higher-frequency linear array can be used to evaluate thin or pediatric patients and to examine bowel adjacent to the abdominal wall in greater detail. The bowel should be evaluated in a systematic fashion with the patient supine. 2/ One technique is described as the “lawn mower” pattern ( Fig. 21.3 ). In this method, A/ begin in (RLQ) the right lower quadrant with the probe held in a B/ transverse orientation (indicator directed to the patient’s right) C/ and scan superiorly toward the right upper quadrant (RUQ). D/ The probe is then moved slightly medially and now scanned inferiorly, parallel to the original path. This pattern is repeated until the whole abdominal surface has been covered.
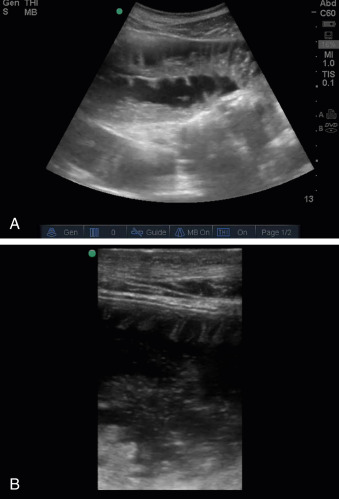
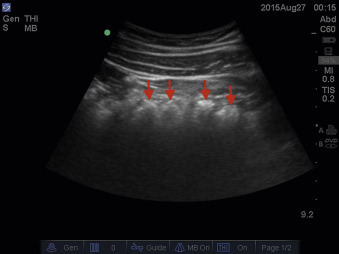
Fig. 21.3 Projected path of the probe when evaluating bowel. The bowel is examined in a systemic fashion, which is sometimes described as a “lawn mower pattern.” As the sonographer moves the probe across the abdomen, 3/ he or she will hold steady, consistent, posteriorly directed pressure into the abdomen at 1- to 2-cm intervals. This technique, known as graded compression, is performed in an attempt to A/ disperse bowel gas and to bring the B/ probe closer to the abdominal contents by compressing abdominal wall soft tissue toward muscular structures of the back. The bowel is often filled with gas. (This gas creates a shadow artifact that prevents visualization of any structures posterior to this artifact. This shadow is typically of mixed echogenicities (“dirty shadow”), as opposed to the typically anechoic shadows (“clean shadow”) of bone or calcium stones. 4/ However, bowel can be visualized when it is filled with liquid, semisolid, or solid material. The 5/ duodenum is difficult to see on ultrasound, but a transverse segment can be seen on the caudal edge of the liver ( Fig. 21.4 ). 6/ The jejunum contains plicae circulares seen 3 to 5 mm apart. This can create a “feather-like” or “herring-bone” appearance ( Fig. 21.5 ).7/ The ileum has fewer of these mucosal folds and may have a smooth appearance. At the terminal ileum, a hypoechoic “halo” may be seen representing the muscular lips of the ileocecal valve. These sonographic findings should be combined with the anatomic location of the bowel to determine the bowel loop under examination. The appendix will be discussed in the next section.
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: small bowel obstruction الخميس مايو 09, 2024 8:55 am
Fig. 21.4 Sonographic image of the duodenum. The duodenum is seen posterior to the gallbladder on the caudal edge of the liver. Fig. 21.5 Sonographic image of the jejunum. jejunum contains a high density of mucosal folds known as plicae circulares (A).These are demonstrated in higher resolution with a high-frequency linear probe (B). The 1/ large bowel has a similar appearance to the small bowel but is distinguished by periodic indentations every 3 to 5 cm apart corresponding to haustral sacculations ( Fig. 21.6 ).2/ The large bowel does NOT contain plicae circulares.3/ The colon can usually be evaluated from the cecal pole to the rectum. The 4/ transverse and descending colon may be difficult to examine, given A/ the variable location (TR colon) B/ and abundant echogenic fat surrounding the lumen (descending colon), respectively. Valves of the rectosigmoid colon and rectum may be visible when the lumen is filled with fluid. Again, correlate the sonographic findings with the anatomic location (paracolic regions) to determine the loop under examination. Fig. 21.6 Sonographic image of large bowel. The large bowel has periodic indentations in the wall, creating segments known as haustra ( arrows ). The air-filled transverse colon is demonstrated here.
Small Bowel Obstruction
The 1/hallmark finding of small bowel obstruction (SBO) is fluid-filled, dilated loops of bowel. The small bowel is 2/ considered dilated when greater than 25 mm in diameter ( Fig. 21.7 ). Some studies use a lower threshold for the ileum (15 mm). Some studies include a required length of dilated bowel.3/ Other findings include 4/ collapsed bowel distal to the areas of dilation or 5/absent/decreased peristalsis distal to the obstruction and the 6/presence of peristalsis in the dilated loops. In a recent meta-analysis by Gottlieb et al., the pooled sensitivities and specificities of ultrasound for the diagnosis of SBO were 92% and 97%, respectively. 7/ Another finding is the “to-and-fro” sign, where intraluminal contents are seen in real time first moving distally, and seconds later the same echoes are visualized moving proximally in the direction from which they originated. Small bowel is approximately 1.5 centimetres (5⁄8 inch) in diameter in newborns after 35 weeks of gestational age, and 2.5–3 cm (1–1+1⁄8 in) in diameter in adults. On abdominal X-rays, the small intestine is considered to be abnormally dilated when the diameter exceeds 3 cm. he normal length of small bowel in an adult, starting from the duodenojejunal flexure, measures between 275 to 850 centimeters. Around 9 liters of fluid passes through the small bowel daily in the form of oral fluids, saliva, gastric, biliary, and pancreatic secretions. Fig. 21.7 Dilated small bowel. Long-axis sonographic image of dilated small bowel measuring 3.5 cm (35 mm) concerning for small bowel obstruction. Above this is bowel containing fluid and semisolid contents. https://radiologykey.com/lower-abdomen-and-bowel/
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Large bowel obstruction الخميس مايو 09, 2024 9:25 am
Ileus
Criteria differentiating ileus from SBO have not been well established. One group suggests that the presence of 1/ dilated small bowel loops with 2/ abundant gas and 3/ the absence of peristalsis with 4/ a colon filled with gas, fluid, or stool is suggestive of ileus. There have been case reports of ultrasound demonstrating gallstone ileus.
Large Bowel Obstruction
Large bowel obstruction (LBO) is also defined by 1/ dilated bowel with a cutoff of greater than or equal to 50 mm 2/ located proximal to normal or collapsed large bowel.3/ The bowel is filled with dense spot echoes and located 4/ on the periphery of the abdomen ( Fig. 21.8 ) 5/ surronding free fluid. Fig. 21.8 Large bowel obstruction. The large bowel is dilated and contains dense echoes in the lumen concerning for large bowel obstruction. There is surrounding free fluid.
Strangulation of Bowel
Strangulated bowel loops will be 1/ dilated and lack peristalsis. According to Schmutz and colleagues, as opposed 2/ to ileus, the distal bowel loops will be collapsed,3/ and the colon will lack intraluminal contents. The 4/ bowel wall may become A/ thickened (>3 mm) and B/lose its mucosal folds ( Fig. 21.9 ). There may be 5/ intraperitoneal fluid around the dilated loops of bowel. This free fluid may form a triangular wedge, termed the tanga sign after a similarly shaped bikini (see Fig. 21.9 ). Fig. 21.9 Strangulated bowel. Multiple, dilated bowel loops with thickened walls (>3 mm) with surrounding intraperitoneal fluid suggestive of bowel strangulation. Note the triangular wedge of intraperitoneal fluid also known as a tanga sign( arrow ).
Etiologies of Bowel Obstruction
Although adhesions are one of the most common etiologies of bowel obstruction, this cannot be visualized using ultrasound. However, other etiologies may be seen, including intussusception, external incarcerated hernias, tumors of the bowel, and gallstone ileus. https://radiologykey.com/lower-abdomen-and-bowel/
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Appendix الخميس مايو 09, 2024 10:30 am
Appendix
Clinical Correlation
Patients may present with acute or chronic (RLQ) right lower quadrant abdominal pain. Etiologies of this pain can be from several different organ systems, including intestinal, urologic, and genitourinary conditions ( Box 21.1 ). One entity that should be considered is appendicitis. Ultrasound may be used as the initial or even definitive modality of imaging to confirm this diagnosis. However, ultrasound findings can sometimes be indeterminate, or visualization of the appendix may not be possible. In these cases, computed tomography (CT) or magnetic resonance imaging (MRI) may be required and can lead to alternative diagnoses. BOX 21.1 Potential Etiologies of Right Lower Quadrant Abdominal Pain
Appendicitis
Ureterolithiasis or renal obstruction (see Chapter 19 )
Inguinal or abdominal wall hernia
Referred pain from testicular pathology: testicular torsion, epididymitis-orchitis, etc. (see Chapter 22 )
Ovarian or adnexal pathology (see Chapter 23 )
Ectopic pregnancy or other pregnancy-related condition (see Chapter 24 )
Normal Anatomy
The 1/ normal appendix is 6 to 9 cm in length. It is an 2/ oval-shaped structure with defined layers (serosa, muscularis, submucosa, mucosa) and is typically less than 6 mm in diameter.3/ The appendix is a blind-looped, vestigial organ that arises off the cecum. 4/ It is classically described as being located at McBurney’s point, which is one-third the distance from the anterior-superior iliac spine (ASIS) and the umbilicus on surface anatomy.5/ (Autopsy and imaging studies) have demonstrated that the appendix is found at this location in only 30% to 40% of patients and is more likely to be oriented in a retrocecal location (up to 65%). 6/ The appendix will often lie superficial to the psoas muscle or iliac vessels ( Fig. 21.10 ). 7/ The normal appendix A/ lacks peristalsis and B/ will collapse with compression. Fig. 21.10 Transverse image of the right lower quadrant of the abdomen. This transverse image using a low-frequency curvilinear probe demonstrates landmarks for identifying the appendix, including the psoas ( P ) and iliac vessels ( arrowheads ). Also seen is a portion of ileum ( arrow ).
Ultrasound Techniques and Normal Findings
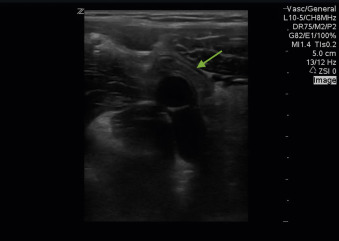
Imaging of the appendix is typically performed using a 1/ high-frequency linear array transducer (typically 9–12 MHz). However, in patients with more abdominal wall soft tissue, the curvilinear probe (typically 3–6 MHz) may be required for further penetration but comes at the expense of lower resolution. The patient is most commonly in the 2/ supine position during examination. However, a recent study shows promise that dynamic patient positioning can increase visualization of the appendix. One approach to finding the appendix is to begin the examination by 3/ placing the probe where the patient reports maximal pain. This region is then evaluated using graded compression, which involves A/ slow, steady pressure into the abdomen using the transducer. This technique will B/ decrease the distance between the appendix and the probe, C/ as well as dissipate bowel gas and its problematic shadow artifact. The examination is continued in a systematic fashion in the right lower quadrant of the abdomen until the appendix is visualized. 4/ Once a loop of bowel is identified as probable appendix, it is critical to trace this segment to confirm that it is blind-ending ( Fig. 21.11 ). Otherwise, a loop of small bowel can be mistaken for the appendix.5/ The appendix is often found overlying the right psoas muscle or the iliac vessels. Once the appendix is identified,6/ it should be visualized in both its long and short axes ( Fig. 21.12 ).7/ The diameter of the appendix should be measured from outer wall to outer wall at its maximal thickness.8/ An attempt should be made to compress the appendix. Color Doppler may be used as an adjunct as is described later. Fig. 21.11 Ultrasound image of the normal appendix demonstrating its blind end. This image shows a long-axis view of the appendix ( arrow ) located anteriorly to the iliac artery.
next
د.كمال سيد Admin
عدد المساهمات : 2464نقاط : 4252السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: Appedicitis imaging & pathology الخميس مايو 09, 2024 10:33 am
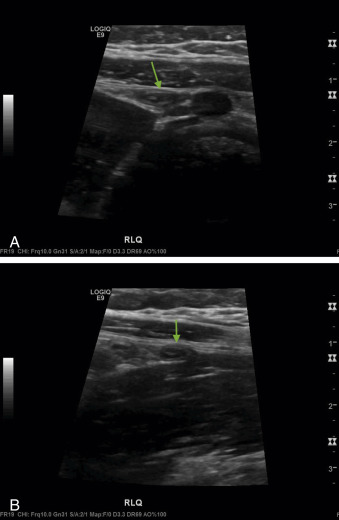
Fig. 21.12 Ultrasound images of the normal appendix in (A) long-axis and (B) in short-axis views ( arrow ). If the appendix cannot be found in the prior manner, an alternative technique can be used :9/ Begin in the right upper quadrant (URQ) with the probe indicator in a cranial orientation and identify bowel gas and haustra from the ascending colon. Again, bowel gas has a hyperechoic stripe superficially with a “dirty shadow” (mixed echogenicity shadow) posteriorly. The 10/ probe is then A/slid caudally toward (RLQ) the right lower quadrant, following the previously identified bowel gas. B/ At the inferior end of the ascending colon, a transition point is encountered where bowel gas ends and abdominal contents are now able to be visualized ( Fig. 21.13 ). This represents the border of the cecum. Now that the cecum is identified, C/ the probe is then moved in a medial and superior fashion to identify the appendix as it arises from the cecal pouch. Fig. 21.13 Ultrasound image of the edge of the cecal pouch. The probe is moved from the right upper quadrant down to right lower quadrant tracing the path of the ascending colon. At the edge of the cecum there is a transition between bowel gas and abdominal contents ( arrow ). Visualization of the appendix is not only a technically challenging study for the operator but is also very dependent on patient factors such as body habitus and ability to comply with the examination. Obesity will add layers of soft tissue between the abdominal wall and the appendix, decreasing resolution and the ability to perform adequate graded compression. Appropriate analgesics before scanning is important so that the patient can tolerate the additional abdominal wall pressure during the graded compressions. If the appendix is not visualized using ultrasound, CT or MRI (pediatric, pregnant) may be necessary.
Pathology
Appendicitis
The hallmark imaging features of an inflamed appendix are (1) a dilated appendix that is greater than 6 mm in diameter and (2) is noncompressible ( Fig. 21.14 ). Again, it is of critical importance that 3/ the appendix is confirmed as having a closed (blind end), as small bowel can easily be mistaken for the appendix on ultrasound imaging.4/ The appendix should be visualized to its distal end, as appendicitis localized to the distal tip has been described. Other potential findings 5/ include periappendical fluid ( Fig. 21.15 ), which is an anechoic stripe or wedge adjacent to the appendix,6/ or periappendical fat stranding ( Fig. 21.16 ). Fat stranding has a similar appearance to early edematous soft tissue (see Chapter 27 ). Fat stranding will be homogenous, hyperechoic haziness with loss of its naturally distinctive layers. Color Doppler may be used as an adjunct. 7/ When visualized in its short axis, the inflamed appendix will demonstrate increased flow circumferentially along its wall and give it a “ring of fire” appearance ( Fig. 21.17 ). https://radiologykey.com/lower-abdomen-and-bowel/








 الخميس فبراير 28, 2013 8:10 pm
الخميس فبراير 28, 2013 8:10 pm