عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: RENAL US الأحد فبراير 10, 2013 5:17 am
RENAL ULTRASOUND
Renal Ultrasound
ultrasound study RENAL CALCULI vs RENAL CONCRETIONS - 1 of 2
ultrasound study RENAL CALCULI vs RENAL CONCRETIONS - 2 of 2
د.كمال سيد Admin
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US الأحد فبراير 10, 2013 8:44 pm
Renal Ultrasound - Hydronephrosis - SonoSite, Inc.
RENAL ULTRASOUND QUESTIONS 1.wmv
RENAL ULTRASOUND QUESTIONS 2.wmv
RENAL ULTRASOUND QUESTIONS 3.wmv
د.كمال سيد Admin
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US الأحد فبراير 10, 2013 8:56 pm
How to: Kidney Ultrasound Exam
How to: Female Transvaginal Ultrasound Exam
3D How To: Right Kidney Ultrasound - SonoSite Ultrasound
3D How To: Left Kidney Ultrasound - SonoSite Ultrasound
د.كمال سيد Admin
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US الإثنين فبراير 11, 2013 5:23 am
Ultrasound for KIDNEY STONE
ultrasound study RENAL CALCULI vs RENAL CONCRETIONS - 1 of 2
ultrasound : calculus in proximal ureter 1 of 2
د.كمال سيد Admin
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: short notes الثلاثاء أبريل 09, 2024 9:19 pm
The renal arteries are the only vascular supply to the kidneys. They arise from the lateral aspect of the abdominal aorta, typically at the level of the L1/L2 intervertebral disk, immediately inferior to the origin of the SMA. They are approximately 4 to 6 cm long, have a diameter of 5 to 6 mm, and run in a lateral and posterior course due to the position of the hilum. They run posterior to the renal vein and enter the renal hilum anterior to the renal pelvis. The renal artery also supplies the adrenal gland and ureter on the ipsilateral side. RRA The right renal artery originates from the anterolateral aspect of the aorta and runs in an inferior course behind (posterior to) the IVC to reach the right kidney, while the left renal artery originates sligh… LRA The left renal artery has a much shorter course and runs slightly more inferiorly compared to the right renal artery. The left renal artery has a more horizontal course and can be found just posterior to the left renal vein before it enters the hilum of the left kidney. Anteriorly, the proximal portion of the right renal artery is related to inferior vena cava, while the distal portion is related to the shorter right renal vein. These structures separate it from the second part of the duodenum and head of the pancreas. Posteriorly, it is associated with the right renal pelvis and the ureter in its distal section whereas, the right crus of the diaphragm, right psoas major muscle, right sympathetic trunk, cisterna chyli, and body of the 2nd lumbar vertebra in its proximal part. The left renal vein separates the left renal artery from the body and tail of the pancreas and the splenic vessels. Posteriorly, its proximal part is related to the left crus of the diaphragm, left psoas major muscle, left sympathetic trunk, and the body of the second lumbar vertebra. The distal portion is related to the left renal pelvis and the ureter, posteriorly.
د.كمال سيد Admin
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US الثلاثاء أبريل 09, 2024 9:41 pm
The renal arteries are the only vascular supply to the kidneys. They arise from the lateral aspect of the abdominal aorta, typically at the level of the L1/L2 intervertebral disk, immediately inferior to the origin of the SMA. They are approximately 4 to 6 cm long, have a diameter of 5 to 6 mm, and run in a lateral and posterior course due to the position of the hilum. They run posterior to the renal vein and enter the renal hilum anterior to the renal pelvis. The renal artery also supplies the adrenal gland and ureter on the ipsilateral side. RRA The right renal artery originates from the anterolateral aspect of the aorta and runs in an inferior course behind (posterior to) the IVC to reach the right kidney, while the left renal artery originates slightly higher and from a more lateral aspect of the aorta, and runs almost horizontally to the left kidney. The renal arteries divide before entering the renal hilum into anterior and posterior divisions, which receive approximately 75% and 25% of the blood, respectively. The anterior division further divides into the upper, middle, lower, and apical segmental arteries.. while the posterior division forms the posterior segmental artery. Segmental arteries subsequently divide into lobar, interlobar, arcuate, and interlobular arteries before forming the afferent arterioles which feed into the glomerular capillaries. LRA The LRA has a much shorter course and runs slightly more inferiorly compared to the right renal artery. The LRA has a more horizontal course and can be found just posterior to the left renal vein before it enters the hilum of the left kidney. Knowledge of the anatomic relations is essential for the surgeons as important structures can suffer an injury during different surgical procedures that require an approach to the renal arteries. Anteriorly, the proximal portion of the RRA is related to IVC, while the distal portion is related to the shorter right renal vein. These structures separate it from the second part of the duodenum and head of the pancreas. Posteriorly, it is associated with the right renal pelvis and the ureter in its distal section whereas, the right crus of the diaphragm, right psoas major muscle, right sympathetic trunk, cisterna chyli, and body of the 2nd lumbar vertebra in its proximal part. The LRV separates the LRA from the body and tail of the pancreas and the splenic vessels. Posteriorly, its proximal part is related to the left crus of the diaphragm, left psoas major muscle, left sympathetic trunk, and the body of the second lumbar vertebra. The distal portion is related to the left renal pelvis and the ureter, posteriorly.
د.كمال سيد Admin
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US السبت أبريل 27, 2024 11:14 am
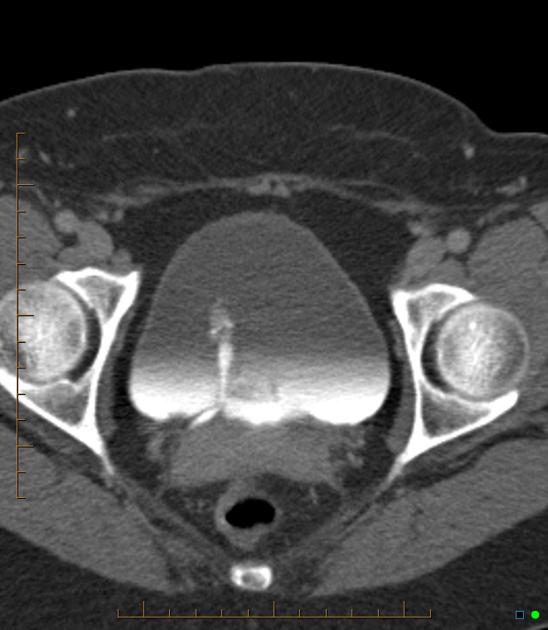
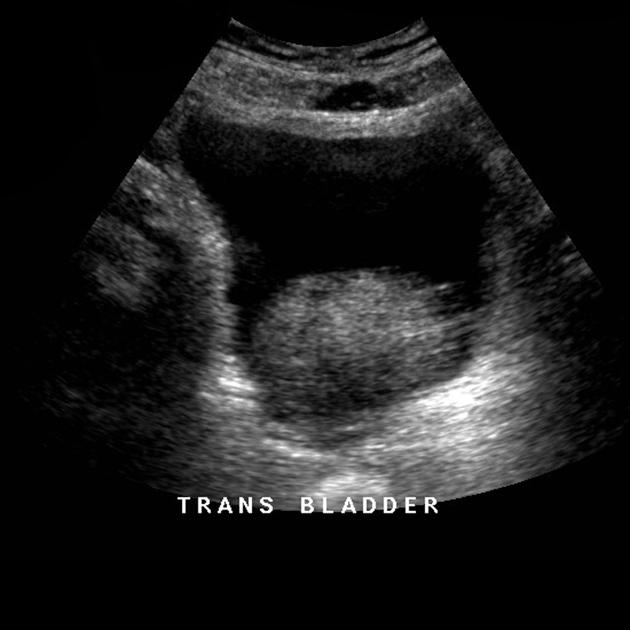
Urinary bladder Urinary bladder The urinary bladder (more commonly just called the bladder) is a distal part of the urinary tract and is an extraperitoneal structure located in the true pelvis6. Its primary function is as a reservoir for urine The pelvic outlet also called the inferior pelvic aperture, defines the lower margin of the lesser (true) pelvis. The pelvic cavity (the true pelvis) predominantly contains 1/ the urinary bladder,2/ the colon, and 3/ the internal reproductive organs. This space is enclosed between the pelvic inlet and the pelvic outlet.
Gross anatomy
The bladder has 1/ a triangular shape with 2/ a posterior base (fundus),3/ superior dome,4/ anterior apex, and 5/ an inferior neck with 6/ two inferolateral surfaces 6.7/ It is lined with a rough, trabeculated transitional cell epithelium, except at the trigone6. The apex (anterior) of the bladder is directed behind the symphysis pubis6, connected to the anterior abdominal wall and umbilicus through the median umbilical ligament (remnant of the embryological urachus) 6, which is covered by the median umbilical fold formed by the overlying peritoneum. The trigone is a triangular area of smooth mucosa lined by stratified squamous epithelium on the internal surface of the base. The superolateral angles are formed by the ureteric orifices and the inferior angle is formed by the internal urethral orifice. As men age, the trigone overlying the mid-portion of the central zone of the prostate may start to protrude as the prostate enlarges forming a mild hemispherical elevation proximal to the internal urinary sphincter, which is called the uvula of the bladder 5. The urethra arises from the neck of the bladder and is surrounded by the internal urethral sphincter. The urethra is separated from the symphysis pubis by retropubic fatty space of Retzius6. As the bladder fills with urine it becomes ovoid and extends superiorly into the abdominal cavity6. Contraction is facilitated by the detrusor muscle The peritoneum over the bladder is relatively loose except at the insertion points of the ureters at the posterior bladder and at the inferior bladder where the peritoneum condensed into pelvic fascia and attached to the pubic bone (pubovesical ligament in females and puboprostatic ligament in males), lateral walls of pelvis and rectum. This makes the inferior part of the bladder relatively fixed. In males, the peritoenum is reflected between the rectum and bladder to form the rectovesical pouch. In females, there are two reflections namely rectouterine pouch (pouch of Douglas) and vesicouterine pouch 6.
sympathetic: reach the pelvic and subsequently the vesical plexus via hypogastric nerves (from the inferior mesenteric ganglion which in turn is supplied by the lumbar splanchnic nerves from the sympathetic lumbar outflow)
parasympathetic: reach the pelvic and subsequently the vesical plexus via pelvic splanchnic nerves (from the parasympathetic sacral outflow)
double bladder: receives ipsilateral ureter and has a separate urethra
septation: septum may divide the bladder internally into two or more compartments
agenesis: persistence of the cloaca
ureterocele: dilation of the intravesical part of the ureter
Radiographic features
The bladder is usually easier to evaluate when full, and it is sometimes difficult to identify when empty. Plain radiographs The bladder may be seen as a rounded soft tissue mass 1. Fluoroscopy Cystography can be performed where the bladder is filled with contrast either via an antegrade or retrograde technique. Ultrasound The bladder wall is best assessed with this modality - it should not exceed 3-5 mm in thickness. Ureteric jets can be assessed using color Doppler ultrasound 1. MRI
T1: bladder wall and contents are homogeneous low signal
T2: bladder wall is of low signal and urine of high signal, allowing for a contrast between the two 1
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US السبت أبريل 27, 2024 12:51 pm
Prostate The prostate gland is the largest accessory gland of the male reproductive system. In adults, the prostate typically weighs ~40 grams with an average size of 3 x 4 x 2 cm15. The prostate comprises 70% glandular tissue and 30% fibromuscular or stromal tissue 1-3 and provides ~30% of the volume of seminal fluid
Gross anatomy
The prostate gland is an inverted pyramid with a base superiorly and apex inferiorly. It has four surfaces: anterior, posterior and two inferolateral surfaces. The base of the prostate is in continuity with the bladder, and the apex ends inferiorly at the urogenital diaphragm1-3. The prostate gland surrounds the proximal urethra, which traverses the prostate close to its anterior surface at the base and then more centrally at the apex. The anterior surface forms the posterior limit of the retropubic space. The prostate is connected to the pubic bone by the puboprostatic ligaments 1. Its inferolateral surfaces rest on the levator ani fascia 3. Its flat triangular posterior surface is anterior to the rectum and has a vertical median groove, which is palpable via a digital rectal exam. The rectovesical fascia (Denonvilliers fascia) separates it from the rectum 13. The seminal vesicles are superior and posterior to the prostate gland. Their ejaculatory ducts pierce the posterior surface below the bladder 1-3 and drain into the prostatic urethra The prostate gland lacks a true capsule, and the so-called prostate capsule is a pseudocapsule formed from fibromuscular tissue surrounding 3 distinct layers of fascia: the anterior, lateral, and posterior fasciae. Anteriorly and apically this pseudocapsule is deficient. Laterally the fascia fuses with the levator fascia. The prostatic venous plexus (of Santorini)lies between and passes through the pseudocapsule
Neurovascular bundles travel posterolaterally at 5 and 7 o'clock and give off branches into the prostate at the apex and base . Zonal anatomy The prostate is comprised of a non-glandular anterior fibromuscular stroma and three distinct glandular zones with different embryologic origins:
peripheral zone
central zone
transition zone
The large cup-shaped peripheral zone (PZ) encompasses the central and transition zones and accounts for approximately 70% of the total prostate volume in a young adult 13. The peripheral zone is deficient anteriorly where it is replaced by the anterior fibromuscular stroma (AFMS) 13. The peripheral zone surrounds the distal prostatic urethra at the apex of the prostate and extends posterolaterally to the base13. The peripheral zone is separated from central and transitional zones by a fibrous layer13. The majority (70%) of prostatic tumors occur in the peripheral zone13. The small wedge-shaped central zone (CZ) 1/ constitutes up 25% of the prostate volume 2/ and contains the ejaculatory ducts 13.3/ It is posterior to the prostatic urethra 4/ and forms the base of the prostate. The smaller transition zone (TZ) makes up the remaining 5% of the prostate volume 13. It surrounds the proximal and middle portions of the prostatic urethra with the bulk of this zone lying anterolateral to the prostatic urethra 2-4. Benign prostatic hypertrophy occurs in the transition zone 13. About 20% of prostatic cancers come from transition zone 13. The transition zone is occasionally written incorrectly as the transitional zone. Superiorly, the anterior fibromuscular stroma is continuous with detrusor muscle. Inferiorly, it blends with levator muscles and puboprostatic ligaments 13. With aging, the central zone atrophies and the transition zone becomes hypertrophic 13. Historically, the prostate was described as having five lobes, the anterior, posterior, median and two lateral lobes. The anterior lobe which joined the two lateral lobes to each other was also known as the isthmus 12. Some radiologists and urologists refer to the central gland (CG) which consists of both the central and transition zones. These zones are discernable on MRI. Relations
additional variable supply by prostatic branches from the middle rectal artery and internal pudendal artery, both of which are branches of the anterior division of the internal iliac artery
Venous drainage
Venous drainage occurs primarily through the prostatic venous plexus into the inferior vesical vein, which in turn drains into the internal iliac vein. Venous blood from the prostatic venous plexus also travels via the Batson venous plexus to drain into the internal vertebral venous plexus2,3,5. The deep dorsal vein of the penis drains into the prostatic venous plexus via its connection with the pudendal venous plexus 3. Therefore, the prostatic venous plexus is a potential route of spreading cancer 13.
Lymphatic drainage
drainage mainly to internal iliac, sacral 13 and obturator nodes
some drainage to external iliac, presacral and para-aortic nodes 1-4
Innervation
The gland is surrounded by the prostatic (nervous) plexus which receives autonomic fibers from the inferior hypogastric plexus:
parasympathetic fibers supplying the inferior hypogastric plexus arise from the pelvic splanchnic nerves (S2-S4) 13
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US الأحد أبريل 28, 2024 6:32 pm
Benign prostatic hyperplasia Benign prostatic hyperplasia (BPH), also known as benign prostatic enlargement (BPE), is an extremely common condition in elderly men and is a major cause of bladder outflow obstruction.
Terminology
The term benign prostatic hypertrophy was formerly used for this condition, but since there is actually an increase in the number of epithelial and stromal cells in the , not an enlargement of cells, the more accurate term is hyperplasia. The term prostate adenoma (plural: adenomas or adenomata) is also often used, as histopathologically the nodular hyperplasia organizes into nodules of =adenoma-general&lang=us]adenoma11. Although the term prostatomegaly is often used synonymously with benign prostatic hyperplasia, strictly speaking prostatomegaly may refer to any cause of prostatic enlargement. Moreover, a significant number of patients with symptomatic benign prostatic hyperplasia do not have enlarged prostates 11. By the same token, benign prostatic enlargement is also a poor term for this condition.
Epidemiology
By the age of 60, 50% of men have benign prostatic hyperplasia, and by 90 years of age, the prevalence has increased to 90%. As such it is often thought of essentially as a "normal" part of aging 1. Risk factors
increasing age
family history
race: Black population > White population > Asian population
Although a degree of prostatomegaly may be completely asymptomatic, the most common presentation is with lower urinary tract symptoms (LUTS) including 1-4:
poor stream despite straining
hesitancy, frequency, and incomplete emptying of the bladder
nocturia
An enlarged prostate may also be incidentally found on imaging of the pelvis or on digital rectal exam. The international prostate symptom score (IPSS) is an 8 question (7 symptom questions + 1 quality of life question) scoring system used in assessing 1/ clinical severity,2/ tracking symptoms, 3/ and aiding management of benign prostatic hyperplasia.
Pathology
Benign prostatic hyperplasia is due to a combination of stromal and glandular hyperplasia, predominantly of the transition zone** (as opposed to prostate cancer which typically originates in the peripheral zone). Androgens (DHT and testosterone) are necessary for the development of benign prostatic hyperplasia but are not the direct cause for the hyperplasia .DHT (dihydrotestosterone) is a hormone that plays a key role in the sexual development of people Assigned Male At Birth (AMAB). More specifically, DHT is an androgen — a hormone that stimulates the development of male characteristics. **BPH mainly arises within the para-urethral transition zone, although BPH adenomas can be seen occasionally in other zones. Markers
Fluoroscopy On IVP, the bladder floor can be elevated and the distal ureters lifted medially (=j-shaped-ureters&lang=us]J-shaped ureters or fishhook ureters). Chronic bladder outlet obstruction can lead to detrusor hypertrophy, trabeculation, and the formation of bladder diverticula. Ultrasound Ultrasound has become the standard first-line investigation after the urologist's finger.
there is an increase in the volume of the prostate with a calculated volume exceeding 30 mL (width x height x length x 0.52)
the central gland is enlarged and is hypoechoic or of mixed echogenicity
calcification may be seen both within the enlarged gland as well as in the pseudocapsule (representing the compressed peripheral zone)
post-micturition residual volume is typically elevated
associated bladder wall hypertrophy and trabeculation due to chronically elevated filling pressures
CT Not typically used to assess the prostate, benign prostatic hyperplasia is more frequently an incidental finding. Extension above the symphysis pubis was used as a marker on axial imaging, however now that volume acquisition and coronal reformats are standard, the same criteria as on ultrasound can be used (>30 mL). MRI
enlarged transition zone
heterogeneous signal with an intact low signal pseudocapsule in the periphery
Treatment and prognosis
Medical management for early disease typically commences with an alpha-blocker such as tamsulosin given in combination with a 5-alpha reductase inhibitor such as dutasteride. Surgical management for symptomatic patients is typically achieved with transurethral resection of the prostate (TURP), and careful patient selection is important given the high prevalence of both benign prostatic hyperplasia and lower urinary tract symptoms (LUTS) in this population. A =prostatic-urethral-lift&lang=us]prostatic urethral lift may be used as intermediate therapy before medication or more invasive TURP 10. Intermittent self-catheterization is an option for those unsuitable for surgery. Other laser procedures can also be used which includes a Holmium laser enucleation of the prostate. Prostatic arterial embolization (PAE) is an emerging minimally invasive procedure which has been shown to have similar efficacy to traditional surgical techniques, with a lower risk of major adverse events such as hemorrhage, urinary tract infection, and sexual dysfunction 9. Urodynamic studies and prostate size estimation are often used to guide therapy, although prostate size in isolation is a poor predictor of symptom severity 4. Complications Complications of untreated benign prostatic hyperplasia include 4:
Despite much debate, it remains unclear if benign prostatic hyperplasia is a risk factor for prostate adenocarcinoma, or if the co-occurrence of the two pathologies is simply an epiphenomenon12.
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US الأحد أبريل 28, 2024 6:53 pm
International prostate symptom score The international prostate symptom score (IPSS) is an 8 question (7 symptom questions + 1 quality of life question) screening tool used in screening, diagnosis, symptom tracking, and aiding management of the symptoms associated with bladder emptying and is useful in those with benign prostatic hyperplasia (BPH) and prostate carcinoma. Score It comprises of Frequency of sensation of not emptying your bladder completely after finishing urinating over a past month
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of having had to urinate again less than 2 hours after finishing urinating in over the past month
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of having to stop and start again several times when urinating over the past month?
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of having found it difficult to postpone urination over the past month,?
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of having had a weak urinary stream over the past month,?
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of having had to push or strain to begin urination over the past month?
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of you most typically getting up to urinate from the time since going to bed at night until the time of getting up in the morning over the past month,?
none (0 points)
1 time (1 point)
2 times (2 points)
3 times (3 points)
4 times (4 points)
5 or more times (5 points)
Over the past month, how often have you had a sensation of not emptying your bladder completely after you finished urinating?
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Over the past month, how often have you had to urinate again less than 2 hours after you finished urinating?
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Over the past month, how often have you found you stopped and started again several times when you urinated?
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of difficulty in postponing urination over the past month
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of weak urinary stream over the past month
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
Frequency of having to had to push or strain to begin urination over the past month
not at all (0 points)
less than 1 time in 5 (1 point)
less than half the time (2 points)
about half the time (3 points)
more than half the time (4 points)
almost always (5 points)
The number of times needed to typically get up to urinate from the time since going to at night until the time you got up in the morning over the past month
none (0 points)
once (1 point)
twice (2 points)
3 times (3 points)
4 times (4 points)
5 or more times (5 points)
Correlation
score: 0-7 = mildly symptomatic
score 8-19 = moderately symptomatic
score 20-35 = severely symptomatic
Prostate specific antigen
Prostate specific antigen (PSA) is currently used as a tumor marker for prostate adenocarcinoma. PSA is a 33 =dalton&lang=us]kilodaltonglycoprotein produced in prostate epithelial cells. Its normal physiologic role is as a liquefying agent for seminal fluid; only a tiny amount leaks into the blood, therefore its normal serum level is usually very low. Elevated serum levels of PSA have been associated with prostate carcinoma. Prostate specific antigen can exist in the serum in two forms:
bound/complexed (to serum protein): elevated levels are associated with prostate cancer
Although an increased PSA level is associated with prostate cancer, a low level cannot exclude prostate cancer. Although exact cut-off values are continually in flux, subject to the most recent data:
2-4ng/mL: 15-25% change in a man >50 years old of having prostate cancer
4-10ng/mL: imaging screening/biopsy indicated
The absolute level may also be misleading if there is a trend in the data upward (or downward) over time. Men with enlarged glands from benign prostatic hyperplasia may also have elevated PSA levels. False-positive levels have been associated with:
An upward trend in a patient's PSA value is usually concerning after a prostatectomy, raising suspicion for recurrent/metastatic disease. Long term (> 6-12 months) treatment with 5α-reductase inhibitors (e.g. finasteride, dutasteride) tends to reduce the PSA level by about 50% 6.
PSA in women
Prostate specific antigen was at one time thought to be only secreted from the prostate, but it is now clear that it is also secreted by cells in women, in particular the breast. The normal serum PSA level in females is approximately 1,000 times less than in men 4,5. PSA is synthesized by both healthy and pathological breast tissue, and studies suggest that an elevated serum PSA, may point towards a favorable prognosis in breast cancer and be useful in monitoring treatment response 4,5.
History and etymology
It was Richard J. Ablin, PhD and professor of pathology in 1970 who discovered the prostate specific antigen 7.
عدد المساهمات : 2461نقاط : 4249السٌّمعَة : 9الجنس : علم بلدك : تاريخ الميلاد : 03/04/1950تاريخ التسجيل : 30/07/2012العمر : 74 الموقع : السودان - سنارالعمل/الترفيه : طبيب عمومى وموجات صوتيةالساعة الان : دعائي :
موضوع: رد: RENAL US الإثنين أبريل 29, 2024 9:22 am
Seminal vesicle The seminal vesicles are paired accessory sex glands of the male reproductive system. The seminal vesicle produces over two-thirds of the ejaculate and is very high in fructose.
Gross anatomy
S.V are leaf like glandular tubular structures with invaginations derived from the dilated end of the ductus deferens (vas deferens)..The vas deferens is felt in the scrotum by first encircling the cord with the fingers and thumb and allowing small amounts of cord tissue to pass between the thumb and second or third fingers until the thick, cordlike vas is felt The vas deferens, or ductus deferens, can be 30 centimeters (almost 12 inches) to 45 centimeters (almost 18 inches) long. Some parts of it are coiled, but other parts are straight. The tube is described as being fibromuscular, meaning that it's made of fibrous tissue and muscle tissue . The seminal vesicle is actually a 10-15 cm (when uncoiled) long tubular structure but is coiled tightly so it only measures 3 to 5 cm in length and 1 cm in diameter.. It is located superiorly and posteriorly to the prostate. The excretory duct of the seminal vesicle unites with the ductus deferens to form the ejaculatory duct. Relations








 الأحد فبراير 10, 2013 5:17 am
الأحد فبراير 10, 2013 5:17 am