
موقع د. كمال سيد الدراوي
طبي_ اكاديمي _ ثقافي _ تعليمي _ _ استشارات طبية_فيديو طبي
|
| | | GB & BILIARY US |  |
| | | كاتب الموضوع | رسالة |
|---|
د.كمال سيد
Admin




عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس : 
علم بلدك : 
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي : 
|  موضوع: GB & BILIARY US موضوع: GB & BILIARY US  الأربعاء أبريل 24, 2024 5:27 pm الأربعاء أبريل 24, 2024 5:27 pm | |
| | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: GB anatomy & S/G الأربعاء مايو 08, 2024 12:33 pm | |
| The GallbladderNormal AnatomyThe normal anatomy of the gallbladder, biliary tract, and surrounding organs is presented in Fig. 17.1 . The gallbladder ( GB) is 1/ connected via the cystic duct to the common hepatic duct ( CHD), forming the common bile duct ( CBD) that drains into 2/ the duodenum through the head of the pancreas. In most situations, 3/ the hepatic artery lies between the CBD and the more posteriorly located portal vein. 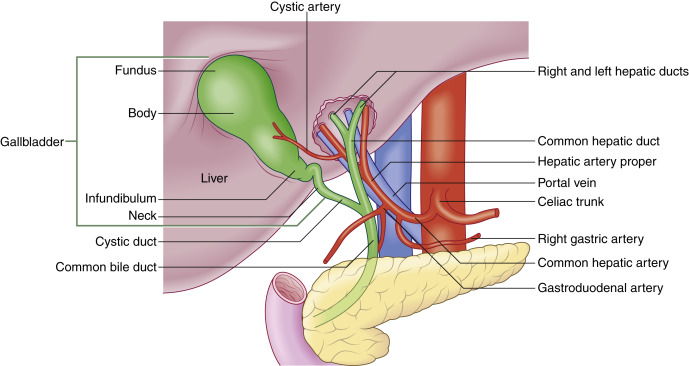 Fig. 17.1 Diagram demonstrating normal anatomy of the upper abdomen, including the relationship of the hepatic artery to the common bile duct and the biliary ductal system. Redrawn with permission from Soni NJ. Point of Care Ultrasound . Philadelphia, PA: Elsevier; 2015:146, Fig. 19.2 . Ultrasound Techniques/FindingsImaging 1/ of the gallbladder is performed using a low-frequency transducer, such as a curved array (typically 3–6 MHz frequency). 2/ It is best to visualize the gallbladder and CBD in a parasagittal, as well as transverse plane, in real time. Patients are often imaged in A/ a supine position; however, turning the patient in a lateral decubitus or right anterior oblique position may improve visualization. Occasionally, placement of the probe in other positions, such as intercostal or through the right flank, may be helpful for gallbladder visualization. Careful and deliberate interrogation of the 3/ entire gallbladder is imperative, as stones may be impacted in the gallbladder neck or pass through the cystic duct into the CBD and cause biliary ductal obstruction. The examiner may find a sonographic Murphy’s sign to be useful. A simple test is performed by placing the probe over the gallbladder to elicit pain. We find that placing the probe in different positions may be best to localize the true site of the pain. Thus probe pressure to the right of the gallbladder, over the gallbladder, and then over the mid-epigastric region may be used to best identify the true site of pain. 4/ A sonographic Murphy’s sign is defined as the presence of maximum tenderness elicited by direct probe pressure over the sonographically located gallbladder. If analgesics have been administered, a Murphy’s sign may be more difficult to elicit. On ultrasound 5/ we are evaluating the gallbladder primarily for A/ stones, signs of inflammation B/ of the gallbladder, C/ and/or biliary obstruction. If the 6/ extrahepatic biliary ductal system appears dilated, then scanning through the liver as well as the head of the pancreas to evaluate the extrahepatic biliary system is important. 7/ It is important to document potential etiologies of biliary ductal obstruction such as c holedocholithiasis and/or distal mass within the pancreas. When there is biliary ductal obstruction but no identifiable etiology on ultrasound, a computed tomography (CT) scan of the abdomen should be performed. Magnetic resonance imaging (MRI) may be useful to better identify etiologies of biliary obstruction such as choledocholithiasis. https://radiologykey.com/gallbladder-and-biliary/ | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Cholelithiasis الأربعاء مايو 08, 2024 3:18 pm | |
| Cholelithiasis and MimicsCholelithiasisThe principal imaging features that distinguish gallstones are 1/ mobility, 2/ echogenic focus, 3/ and acoustic shadowing ( Fig. 17.2 ,   ). Multiple studies have shown sensitivities of ultrasound of approximately 95%, with even higher positive and negative predictive values. Gallstones may also demonstrate a 4/ “twinkle” artifact on color Doppler imaging ( Fig. 17.3 ). When an echogenic focus is identified in the gallbladder, first shadowing should be confirmed. This is followed by repositioning the patient to demonstrate stone mobility. This can include having the patient upright or standing. Stones lodged in the cystic duct may not move. Careful attention to surrounding structures is important, so as not to confuse an echogenic bowel (which can create a “dirty shadow”) with gallstones ( Fig. 17.4 ). This artifact can be differentiated from stones by A/ scanning the patient in different positions and noting that the bowel is B/ NOT within the gallbladder fossa, as well as noting C/ peristalsis within the bowel (  ). Scanning in D/ different planes or obliquely may be necessary to separate adjacent bowel from the gallbladder (see Fig. 17.4 ). E/ A Refraction artifact, which is a mildly echogenic area in the region of the neck of the gallbladder that produces acoustic shadowing, can also be confused for gallstones. F/ This edge artifact is due to refraction or from the multiple small valves of Heister within the cystic duct. Other nonmobile echogenicities within the gallbladder, which may be confused with cholelithiasis, are listed in Table 17.1 .  Fig. 17.2 Cholelithiasis/focal fatty sparing of the liver. Scans through the gallbladder demonstrated multiple echogenic foci ( curved arrow ) with acoustic shadowing ( arrowheads ), which are consistent with gallstones. In addition, there is a focal hypoechoic region noted anterior to the gallbladder ( arrows ), which represents an area of focal fatty sparing in a patient with diffuse fatty infiltration of the liver. From McGahan J. General and Vascular Ultrasound: Case Review . 3rd ed. Philadelphia, PA: Elsevier; 2016:117, Fig. 57-1. 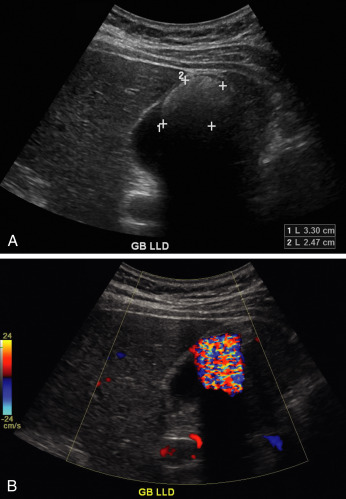 Fig. 17.3 Gallstone with “twinkle” artifact. (A) Large gallstone ( calipers ) in a contracted gallbladder. (B) Color Doppler demonstrates mosaic appearance to the color originating at the anterior surface of the gallbladder, representing the “twinkle” artifact. 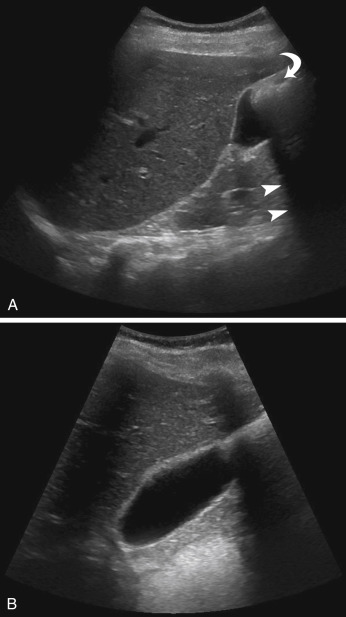 Fig. 17.4 Bowel mimicking gallstones. (A) This longitudinal scan of the liver and gallbladder demonstrates an echogenic focus ( curved arrow ) noted anteriorly within the gallbladder with distal acoustic shadowing ( arrows ). (B) Another scan, using different probe angulation, demonstrates the echogenic focus. This was bowel that moved, and there was no evidence of cholelithiasis. TABLE 17.1 Nonmobile Echogenicities in the Gallbladder That May Shadow - •
Stone lodged in the gallbladder neck
- •
Stone adherent to gallbladder wall
- •
Gallbladder fold
- •
Intramural gas secondary to emphysematous cholecystitis
- •
Adenomyomatosis with stone in Rokitansky–Aschoff sinus
|
The gallbladder is best examined 5/ when the patient is fasting. In emergent situations, the patient may not always be adequately prepped. Thus when the patient is not fasting, the gallbladder may be contracted. Even in these situations, gallstones may be identified. 6/ Also, the gallbladder may be in a permanent state of contraction in cases of chronic cholecystitis. In these situations the Wall, Echo, and Shadow, or “WES,” triad is observed. This corresponds to a visualization of the anterior gallbladder wall, with echogenicity representing the echogenic gallstones and posterior acoustic shadowing ( Fig. 17.5 ,  ). Again, this WES triad is fairly specific for chronic cholecystitis and cholelithiasis, but in patients with gallstones who are not fasting, their gallbladder may have a similar appearance. “Twinkle” artifact can also be seen in this entity (see  ). Patients with porcelain gallbladders will have an echogenic gallbladder wall with some shadowing. A porcelain gallbladder may predispose a patient to gallbladder cancer. 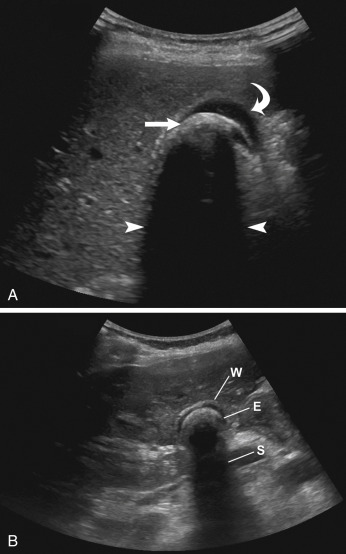 Fig17.5 Wall echo shadow ( WES) triad. (A) Transverse image demonstrating anterior gallbladder wall ( curved arrow ) and partially collapsed gallbladder surrounding a large gallstone ( arrow ). Posterior to this there is an echogenic focus with acoustic shadowing ( arrow heads ) representing a large gallstone. There is still some fluid within the gallbladder. (B) In another patient, there is a near completely contracted gallbladder with anterior gallbladder wall ( W ) surrounding the gallstone as an echogenicity ( E ) and distal acoustic shadowing ( S ), giving the WES appearance. https://radiologykey.com/gallbladder-and-biliary/ | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Sludge الأربعاء مايو 08, 2024 3:54 pm | |
| Cholelithiasis Mimic: SludgeTumefactive sludge ( tumefactive : any lesion causing swelling) Biliary sludge is 1/ a mixture of particulate solids that have precipitated from bile. Such sediment consists of 2/ A cholesterol crystals, B/ calcium bilirubinate pigment, C/ and other calcium salts. It is often an 3/ incidental finding when there is US examination of the gallbladder in a patient with right upper quadrant pain. 4/ Tumefactive biliary sludge may mimic gall stones or a mass. 5/ However, sludge will not shadow. BUT If gallstones are surrounded by sludge, they may produce the “twinkle” artifact or shadowing, thus can be an exception to the rule of no acoustic shadowing with sludge 6/ Often this sludge may be mobile ( Fig. 17.6 ). Thus with repositioning of the patient, sludge may move. Additionally, adding color or power Doppler to the evaluation should 7/ demonstrate lack of vascularity in the sludge. Other causes of gallbladder masses and mimics of cholelithiasis are listed in Table 17.2 . 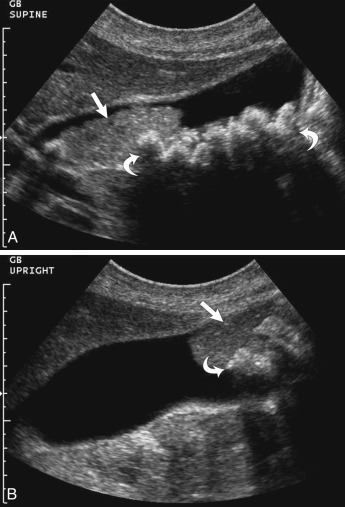 Fig. 17.6 Biliary sludge and cholelithiasis. (A) To the left side of the image there is an echogenic mass ( arrow ) without shadowing within the gallbladder lumen representing gallbladder sludge. To the right, there are multiple echogenic foci ( curved arrows ) with acoustic shadowing, representing gallstones. (B) When the patient is placed in an upright position, this mass ( arrow ) is mobile and falls to the dependent portion of the gallbladder. Note: Multiple echogenicities ( curved arrow ) within this echogenic sludge represent the gallstones. TABLE 17.2 Cholelithiasis and Possible MimicsEchogenic layer with acoustic shadowing = Multiple stones Usually dependent, no color. Often mobile = Sludge/sludgeball Stones surrounded by sludge (as above). = Stones and sludge Blood = Dependent in gallbladder /or fills entire gallbladder. No shadowing. Pus = Similar to blood, but with finding of acute cholecystitis Pseudo-sludge = A curvilinear echogenicity whose borders may project beyond the gallbladder and may disappear with different transducer orientations Parasites = Only in endemic areas or in patients from these areas Gallbladder polyps = Small masses with or without color flow. Gallbladder cancer = Gallbladder mass with color flow and wall thickening, and often gallstones. https://radiologykey.com/gallbladder-and-biliary/ | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Gallbladder Masses: Polyps/Cancer الأربعاء مايو 08, 2024 5:57 pm | |
| Gallbladder Masses: PolypsBoth benign and malignant gallbladder masses may be encountered when examining the gallbladder in the acute setting. This includes gallbladder polyps, cancer, or, rarely, metastasis ( Fig. 17.7 ,  ). Most polyps are small and may resolve spontaneously. However, adenomatous polyps may be precancerous. 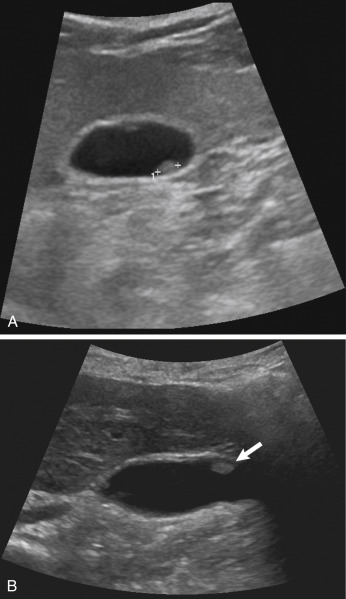 Fig. 17.7 Gallbladder polyps. (A) This image demonstrates an echogenic focus without shadowing ( calipers ) in the dependent portion of the gallbladder, representing a gallbladder polyp. If proper technique was not used, this could be misinterpreted as a gallstone. (B) In another patient, there is an anterior echogenic focus ( arrows ) without acoustic shadowing, representing a gallbladder polyp. Gallbladder CancerGallbladder cancer may be missed on routine ultrasound. This is probably due to the fact that gallstones are often present in patients with gallbladder cancer, and any mass within the gallbladder may be obscured by the gallstones. Gallbladder carcinoma 1/ can be echogenic, isoechoic, or hypoechoic, and 2/ usually does have color Doppler flow. 3/ Gallbladder cancer may cause either diffuse or focal thickening of the gallbladder wall ( Fig. 17.8 ). Primary gallbladder cancer 4/ may invade the adjacent liver. 5/ Various cancers, including melanoma and gastrointestinal ( GI) cancers, may metastasize to the gallbladder and appear as a vascular GBr mass.  Fig. 17.8 Gallbladder carcinoma. Longitudinal scan of the gallbladder demonstrates a gallstone ( curved arrow ) with a nonmobile mass ( arrow ) in the gallbladder. There is also gallbladder wall thickening. An ill-defined mass ( arrowheads ) in the liver represents local invasion into the liver from the gallbladder adenocarcinoma. AdenomyomatosisAdenomyomatosis is characterized by 1/ epithelial proliferation and 2/ mucosal diverticula called Rokitansky–Aschoff sinuses. The most common form creates 3/ localized and confined wall thickening at the fundus of the gallbladder. This thickening can be so great, it appears as a mass and may be hard to distinguish from gallbladder cancer. There are other rare forms of segmental or diffuse adenomyomatosis. 4/ The pathognomonic finding of adenomyomatosis is the presence of hyperechoic foci, most commonly noted in the anterior wall of the gallbladder, which produces a comet tail artifact that decreases in width and amplitude more posteriorly ( Fig. 17.9 ,   ). This is thought to be secondary to cholesterol crystals within the Rokitansky–Aschoff sinuses in the gallbladder wall. 5/ Color Doppler will show a “t winkle artifact” in this entity (see Fig. 17.9 ), which is similar to the “twinkle” artifact seen with gallstones. 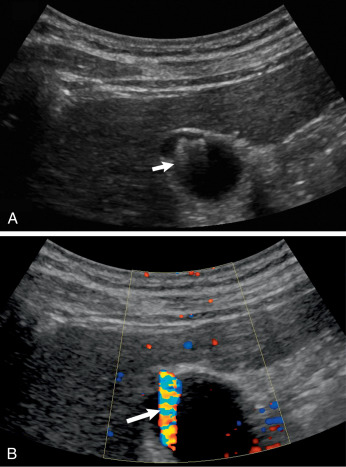 Fig. 17.9 Adenomyomatosis. (A) Transverse scan through the gallbladder demonstrates a few echogenic foci with “ring-down artifact” ( arrow ). Note this is different than in cholelithiasis, where there is acoustic shadowing. (B) In the same region there is “twinkle” artifact ( arrow ), which can be seen with both adenomyomatosis and cholelithiasis. Acute Right Upper Quadrant PainThe American College of Radiology has imaging criteria for patients with right upper quadrant pain who have fever, leukocytosis, and a clinical positive Murphy’s sign, and recommends ultrasound as the first-line test in these situations ( Table 17.3 ). Patients may present with acute or chronic pain in the right upper quadrant of the abdomen. The level and acuity of pain are secondary to the etiology of the pain. For instance, chronic pain may be secondary to chronic cholecystitis and cholelithiasis, whereas more acute pain may be secondary to acute cholecystitis, gallbladder perforation, or acute biliary obstruction. Abnormalities of the liver, biliary tract, pancreas, or kidney should be considered in the differential as listed in Table 17.4 . In some situations, the etiology of the pain may not be discovered or may be secondary to etiologies that may require other imaging, such as CT. Potential Etiologies of Right Upper Quadrant Pain, Including Those Due to Gallbladder Disease, Biliary Disease, or Disease in Surrounding Organs
Cholelithiasis
Acute calculus cholecystitis
Acute acalculous cholecystitis
Complications of acute cholecystitis
Biliary obstruction
Pancreatic mass (see Chapter 18 )
Pancreatitis (see Chapter 18 )
Hepatitis, hepatic abscess/mass (see Chapter 16 )
Pyelonephritis or renal obstruction (see Chapter 19 )
Renal colic/abscess (see Chapter 19 )
Gastroenteritis/colon disease
Abdominal aortic aneurysm
Right lower lobe pneumonia
No identified etiology
|
https://radiologykey.com/gallbladder-and-biliary/ | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Gallstones الخميس مايو 09, 2024 1:22 pm | |
| GallstonesGallstones, also called cholelithiasis, are concretions that may occur anywhere within the biliary system, most commonly within the gallbladder. TerminologyGallstones (cholelithiasis) describe stone formation at any point along the biliary tree. Specific names can be given to gallstones depending on their location: - cholecystolithiasis: gallstones within the gallbladder
- the terms cholelithiasis or gallstones have been largely used in clinical practice on their own to refer to stones in the gallbladder
choledocholithiasis: gallstones within the bile ducts
Biliary microlithiasis refers to gallstones <3 mm in diameter. The term biliary microlithiasis is occasionally used as a synonym for sludge, however, this is not strictly correct. Sludge may include these microliths in its composition, but these are only one element of a variable mixture of crystals, proteinaceous debris, lysed cells and mucin 12. Risk factorsCholesterol gallstones- female sex
- middle age
- obesity
- positive family history
- recent rapid weight loss
Also see the 5-F rule. Pigment gallstonesbrown pigment stones
infection
bacterial
parasitic (e.g. =clonorchis-sinensis&lang=us]Clonorchis sinensis)
biliary stasis
Clinical presentationGallstones may be symptomatic in only 25% of cases. The most common presentation is with =biliary-colic&lang=us]biliary colic (right upper quadrant or epigastric abdominal pain or discomfort, especially after a fat-rich meal). Other symptoms include belching, bloating, flatulence, heartburn, and nausea. Abdominal pain is often r eferred to the right shoulder. Patients may demonstrate this radiation to the tip of the scapula by placing their hand behind the back and thumb pointing upwards: " Collins sign". This may be useful in distinguishing gallstone pain from esophagitis, gastritis, or duodenal ulcer in ~50% of patients 5. Pathology There are three types of gallstones 3,4,7-10: - cholesterol (10%)
- More than 50% cholesterol contents; form with supersaturation of bile, nucleation (assemblage and merger of bile liquid crystals) and stone growth
- predisposing factors
- diet, sedentary lifestyle, the rapid loss of weight, obesity, oral contraceptive pill, total parenteral nutrition (TPN)
- ethnicity, genetic predisposition, older age, female sex
mixed (80%)
20-50% cholesterol content is
predisposing factor: similar to cholesterol stones
pigment stones (10%)
cholesterol content is less than 20%; high bilirubin content and occur when there is supersaturation of unconjugated bilirubin
two subtypes each with their own predisposing factors:
black pigment stones: chronic hemolysis, cirrhosis, intestinal malabsorption
brown pigment stones: infections (bacterial/parasitic) and biliary stasis
Radiographic featuresPlain radiographSome radiopaque gallstones may be seen on plain film: - gallstones are radiopaque only in 15-20% of cases 3
- may be laminated (a.k.a. lamellated): radiopaque outline with lucent center
- may have a faceted outline
- may show a Mercedes-Benz sign: tri-radiate pattern of gas lucency
- In the gallbladder, the Mercedes-Benz sign describes a star-shaped pattern of gas-fissuring within gallstones initially described on an abdominal radiograph 2. Fissures, usually fluid-filled, are present in close to 50% of gallstones
 Ultrasound UltrasoundUltrasound is considered the gold standard for detecting gallstones 6: - greyscale ultrasound
- highly reflective echogenic focus within gallbladder lumen, normally with prominent posterior acoustic shadowing regardless of pathological type (acoustic shadowing is independent of the composition and calcium content) 11
- gravity-dependent movement is often seen with a change of patient position (the rolling stone sign)
color Doppler
may demonstrate a twinkling artifact and is particularly useful for identification of small stones
CTCalcified gallbladder stones are hyperattenuating to bile, making them the only type to be clearly visualized on CT scan images. On CT, a high percentage of cholesterol stones are hypoattenuating relative to bile 15, and other gallstones are isodense to bile and these may not be clearly identified on CT. Treatment and prognosisExpectant management for patients with incidentally detected asymptomatic gallstones is the recommended approach. Laparoscopic cholecystectomy remains the standard treatment for gallstones. It also can be safely performed during any trimester of pregnancy when indicated 16. Complications Differential diagnosisPossible imaging differential considerations in selected situations include Practical points- gallstone acoustic shadowing is prominent with
- larger size stones (usually >3 mm for shadowing)
- higher transducer frequency
- focal zone at the level of gallstone
a gallbladder full of stones may paradoxically be hard to visualize (wall-echo-shadow sign)
Quiz questionshttps://radiopaedia.org/articles/gallstones-1 | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Cholecystitis الخميس مايو 09, 2024 3:37 pm | |
| Cholecystitis
Cholecystitis refers to any form of inflammation involving the gallbladder and has many forms, including: acute cholecystitis Its epidemiology, clinical presentation, pathology, and radiographic features are dependent on the actual etiology. Acute cholecystitis refers to the acute inflammation of the gallbladder. It is the primary complication of cholelithiasis and the most common cause of acute pain in the right upper quadrant (RUQ). Clinical presentationConstant ( RUQ) right upper quadrant pain that can radiate to the right shoulder. Pain typically persists for more than six hours, in contradistinction to the intermittent ( RUQ) right upper quadrant pain of biliary colic. Nausea, vomiting, and fever are also often reported. Pathology 90to 95 % of cases are due to gallstones (i.e. acute calculous cholecystitis) with the remainder being acute acalculous cholecystitis. The development of acute calculous cholecystitis follows a sequence of events: - gallstone obstruction of the gallbladder neck or cystic duct
- inflammation from chemical injury of the mucosa by bile salts
- reactive production of mucus, leading to increased intraluminal pressure and distention
- increased luminal distention restricting blood flow to the gallbladder wall (gallbladder hydrops)
- Gallbladder hydrops or mucocele refers to marked dilatation of the gallbladder due to chronic obstruction of the cystic duct resulting in accumulation of sterile non-pigmented mucin.
- increasing wall thickness from edema and inflammatory changes
- secondary bacterial infection in ~66% of patients
Radiographic featuresUltrasound (US) is the preferred initial modality in the investigation of right upper quadrant pain. It is more sensitive than HIDA scintigraphy 4 and CT in the diagnosis of acute cholecystitis, and more readily available. UltrasoundThe most sensitive US finding in acute cholecystitis is the presence of cholelithiasis in combination with the sonographic Murphy sign. Both gallbladder wall thickening (>3 mm) and pericholecystic fluid are secondary findings. Other less specific findings include gallbladder distension and sludge. Every effort should be made to demonstrate the obstructing stone in the gallbladder neck or cystic duct.Acute cholecystitis refers to the acute inflammation of the gallbladder. It is the primary complication of cholelithiasis and the most common cause of acute pain in the right upper quadrant (RUQ). Acute Acalculous cholecystitis refers to the development of cholecystitis in the gallbladder either without gallstones or with gallstones where they are not the contributory factor. It is thought to occur most often due to biliary stasis and/or gallbladder ischemia. PathologyAcute acalculous cholecystitis usually occurs in critically ill or injured patients (e.g. trauma, burns, sepsis). The risk factors listed above may affect the perfusion of the gallbladder and favor bile stasis leading to injury and inflammation. Subsequent ischemia-reperfusion injury to the gallbladder is also a central pathogenic feature 2,9. A rare cause of acalculous cholecystitis occurring in patients with advanced cancer is gallbladder metastases 10. Case reports have also described acute acalculous cholecystitis likely precipitated by snake envenomation 16, as well as a presenting feature in a patient with Kawasaki disease 17. UltrasoundMay show 1/ GB wall edema, 2/ pericholecystic fluid, and 3/ GB distention (the first two considered the two most important criteria 2). 4/ The sonographic Murphy sign may be positive.5/ A sonolucent intramural layer or “ halo” that represents intramural edema may also be present. A sonogram may be considered highly suggestive of the diagnosis with two of the following major criteria, or one major and two minor criteria fulfilled 14; minor criteria
echogenic bile or sludge in the lumen
transverse diameter >5 cm
Scintigraphy Scintigraphy (from Latin scintilla, "spark"), also known as a gamma scan, is a diagnostic test in nuclear medicine, where radioisotopes attached to drugs that travel to a specific organ or tissue ( radiopharmaceuticals) are taken internally and the emitted gamma radiation is captured by gamma cameras, which are external detectors that form two-dimensional images [1] in a process similar to the capture of x-ray images. Tc-99m iminodiacetic acid cholescintigraphy is considered a highly reliable test and may be performed even in acutely ill patients. Ideally, there is non-visualization of the gallbladder. Treatment and prognosisThe importance of recognizing acalculous cholecystitis lies in the fact that these patients have a high rate of recurrence when treated with medical management. As such, cholecystectomy is the definitive treatment. However, patients that are not fit for surgery can undergo percutaneous or endoscopic biliary drainage as an alternative therapy, though cholecystectomy may still be performed when the patient improves.    Quiz questionshttps://radiopaedia.org/articles/acute-acalculous-cholecystitis?lang=us
عدل سابقا من قبل د.كمال سيد في الأحد مايو 12, 2024 7:57 am عدل 1 مرات | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Chronic cholecystitis الخميس مايو 09, 2024 3:58 pm | |
| Chronic cholecystitis refers to prolonged inflammatory condition that affects the gallbladder. It is almost always seen in the setting of cholelithiasis ( 95%), caused by intermittent obstruction of the cystic duct or infundibulum, or dysmotility. Clinical presentationPatients may have a history of recurrent acute cholecystitis or biliary colic, although some may be asymptomatic. PathologyMicroscopically, there is evidence of chronic inflammation within the gallbladder wall. Associations - gallbladder dysmotility may be present
- there is a possible association between chronic cholecystitis and infection with Helicobacter pylori
Radiographic featuresThe most commonly observed imaging findings are non-specific cholelithiasis and gallbladder wall thickening 2. The gallbladder may appear contracted or distended, and pericholecystic inflammation is usually absent. Uncomplicated chronic cholecystitis is usually managed with elective cholecystectomy. Complications Recognized complications related to chronic cholecystitis include Gangrenous cholecystitis is the most common complication of acute cholecystitis, affecting ~15% (range 2-30%) of patients. Risk factors PathologyGangrenous cholecystitis occurs as a result of ischemia with necrosis of the gallbladder wall 4. Radiographic featuresUltrasoundIn addition to features of acute cholecystitis, the following may help diagnose gangrenous cholecystitis 3: - intraluminal membranes
- asymmetrical wall thickness
- with possible wall disruption and/or ulceration
focal perfusion defects on Doppler (representing areas of necrosis)
variable absence of the sonographic Murphy sign 7
attributed to ischemic denervation of the gallbladder 6
Mortality is increased compared to uncomplicated acute cholecystitis, estimated at between 15-50% 4.  https://radiopaedia.org/articles/gangrenous-cholecystitis?lang=us https://radiopaedia.org/articles/gangrenous-cholecystitis?lang=us | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Gallbladder perforations الخميس مايو 09, 2024 4:31 pm | |
| Gallbladder perforationsGallbladder perforations are a serious complication of acute cholecystitis and represent an advanced stage of the disease. They tend to occur in an elderly and/or comorbid demographic and carry higher rates of morbidity and mortality. Comorbidity is a medical term that you may have heard your doctor use. It describes the existence of more than one disease or condition within your body at the same time. Comorbidities are usually long-term, or chronic. They may or may not interact with each other. Demographics are statistics that describe populations and their characteristics. Demographic analysis is the study of a population-based on factors such as age, race, and sex. Clinical presentationSymptoms and clinical signs are variable and can range from benign non-specific abdominal symptoms to acute generalized peritonitis. The presentation of gallbladder perforation can be indistinguishable from uncomplicated acute cholecystitis 1. PathologyGallbladder perforation is the result of acute cholecystitis. The sequence of events leading to perforation begins with 1/ occlusion of the cystic duct (most often by a calculus), 2/ with resultant retention of intraluminal secretions.3/ Distention of the GB with a 4/ consequent rise in intraluminal pressure can 5/ impede venous and lymphatic drainage, leading 6/ to vascular compromise and 7/ ultimately to necrosis and perforation of the gallbladder wall. Regarding the timing of onset, perforation can be between two days to several weeks after the onset of acute cholecystitis. Perforation often occurs iatrogenically during laparoscopic cholecystectomy, with an incidence estimated to be 15-30% 3. It can also rarely occur from blunt or penetrating trauma. Classification According to the Niemeier classification, there are three main clinical subtypes 9. A fourth type has been suggested by Andersen et al. 10. - type I: acute free perforation
- type II: subacute pericholecystic abscess
- type III: chronic cholecystoenteric fistulation
- type IV: cholecystobiliary fistula formation
Radiographic featuresUltrasoundUltrasound is the initial investigation of choice. Reported findings include =pericholecystic-fluid&lang=us]pericholecystic fluid collection(s) with layering of the gallbladder wall 8. Treatment and prognosisGallbladder perforation may be initially treated by percutaneous cholecystostomy. Patients typically require intravenous antibiotics, volume resuscitation, and close monitoring in an intensive care unit. Eventually (if possible), cholecystectomy is performed 6. Given that gallbladder perforation represents an advanced stage of acute cholecystitis, typically occurring in otherwise comorbid patients, the prognosis is often worse. Although very high mortality rates of ~40% were initially reported in the 1940s, contemporary literature cites a mortality rate between 12-16% 6. Percutaneous cholecystostomy is the image-guided placement of a drainage catheter into the gallbladder lumen. This minimally invasive procedure can aid in patient stabilization in order to enable a more measured surgical approach with time for therapeutic planning. Reported complications include 1,6:
عدل سابقا من قبل د.كمال سيد في الأحد مايو 12, 2024 8:06 am عدل 1 مرات | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Choledocholithiasis الخميس مايو 09, 2024 7:04 pm | |
| Choledocholithiasis denotes the presence of gallstones within the bile ducts (including the common hepatic duct/common bile duct). EpidemiologyCholedocholithiasis is relatively common, seen in up to 20% of patients undergoing cholecystectomy for gallstone-related complaints 2. Clinical presentationStones within the bile ducts are occasionally asymptomatic and may be found incidentally. However, more frequently they lead to symptomatic presentation with: PathologyStones within the bile duct most commonly pass from the gallbladder but may form in situ. When recurrent, they tend to be pigment stones, and are thought to be associated with bacterial infection 1. Radiographic featuresUltrasoundAlthough ultrasound is usually the first investigation for biliary disease, it has average sensitivity for the detection of biliary stones within the bile duct. Ultrasound should be performed 1/ both longitudinally and transversely through the duct with particular attention paid to the very distal portion of the ( CBD) common bile duct as it passes through the pancreatic head ( best assessed transversely). Findings include: - visualization of stone(s)
- echogenic rounded focus
- size ranges between 2 to >20 mm
- shadowing may be more difficult to elicit than with gallstones within the gallbladder
- Twenty percent of common bile duct stones will not shadow
- twinkling artifact may be useful to detect occult stones
dilated bile duct
More than 6 mm + 1 mm per decade above 60 years of age
More than 10 mm post-cholecystectomy
dilated intrahepatic biliary tree
gallstones should increase suspicion, especially if multiple and small
Endoscopic ultrasonography (EUS) is also used with very high sensitivity and specificity. CT Routine contrast-enhanced CT is moderately sensitive to choledocholithiasis with a sensitivity of 65-88% 3, but it requires attention to a number of potentially subtle findings. These include: - target sign
- central rounded density: stone
- surrounding lower attenuating bile or mucosa
rim sign: stone is outlined by thin rim of high density on contrast-enhanced CT 3
crescent sign: bile eccentrically outlines luminal stone, creating a low attenuation crescent 3
calcification of the stone: only 20% of stones are high density
Setting window level to the mean of the bile duct and setting the window width to 150 HU has been reported to improve sensitivity. Biliary dilatation may also be visible. CT cholangiography CT with prior administration of biliary excreted contrast agents is highly sensitive (88-96%) and specific (88-98%) 8 for choledocholithiasis. The difficulty is, however, two-fold: - contrast agents have relatively high complication rates
- obstructive cholestasis diminishes excretion, and thus is only viable in patients with largely normal liver function tests
MRCP Magnetic resonance cholangiopancreatography (MRCP) has largely replaced ERCP as the gold standard for diagnosis of choledocholithiasis, able to achieve similar sensitivity (90-94%) and specificity (95-99%) 7,8 without ionizing radiation, intravenous contrast, or the complication rate inherent in ERCP. Filling defects are seen within the biliary tree on thin cross-sectional T2 weighted imaging. Care should be taken not to use thick slabs for the diagnosis as volume averaging may obscure smaller stones. However, if the diagnosis has already been secured by ultrasound or CT, there is no additional value of MRCP, and the next step is therapeutic ERCP (see below). Percutaneous or oral cholangiography Both investigations are no longer used for routine diagnosis having been replaced by ultrasound, CT and MRCP. Treatment and prognosisEndoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy is the treatment of choice for choledocholithiasis, however, is associated with a complication rate of 5.8-24% (10 years follow-up) 1. Complications of ERCP and sphincterotomy include: Failure of endoscopic clearance of bile duct stones may require either intraoperative bile duct exploration, or percutaneous biliary drainage to decompress the biliary system to temporise and allow subsequent definitive management. Differential diagnosisThere is usually little differential, and differential will depend on the modality. The most frequent entities to consider include: other filling defects
air bubbles
parasites
mimics
partial volume averaging of bowel gas
vascular calcification
surgical clips
MRCP specific potential pitfalls 6
susceptibility artifacts
flow voids
vascular impressions: pseudostricture of the extrahepatic bile duct due to pulsatile vascular compression of the hepatic and gastroduodenal arteries should not be misdiagnosed as a bile duct stricture, tumor or stone 9
sphincteric contraction or pseudocalculus sign
 ERCP & US    Cholangiogram Quiz questionshttps://radiopaedia.org/articles/choledocholithiasis?lang=us | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Obstructive Jaundice الخميس مايو 09, 2024 7:33 pm | |
| Obstructive Jaundice
Jaundice refers to a clinical sign of hyperbilirubinemia ( serum bilirubin >2.5 mg/dL) which has many causes. It is often a clue to a diagnosis. It can be largely divided into two types: - non-obstructive, i.e. prehepatic and hepatic causes
- obstructive, i.e. posthepatic causes
Imaging has a major role in detecting the obstructive causes. Clinical presentationClinically, jaundice presents with yellowing of the skin, conjunctiva (often incorrectly attributed to the sclerae) 5, and mobile oral tissues (e.g. frenulum, palate) 6. These structures are affected due to their high elastin content, which bilirubin has a high affinity for 6. It may be painless, painful, or pruritic. Painless jaundice is always very suspicious for an underlying obstructive malignant cause 3. PathologyCategories of causes 3: hepatic
acute hepatitis/acute liver failure
cirrhosis
Gilbert syndrome
post-hepatic (or obstructive jaundice)
benign causes
choledocholithiasis
choledochal cyst 7
strictures, e.g. post-inflammatory/infectious, primary sclerosing cholangitis, traumatic or operative
external biliary tree compression, e.g. pancreatic pseudocyst, Mirizzi syndrome
parasites (Ascaris, Clonorchis, Fasciola) 7
malignant causes
portal lymphadenopathy
cholangiocarcinoma
carcinoma of head of pancreas
hepatocellular carcinoma
gallbladder carcinoma
duodenal/ ampullary carcinoma
metastases
Radiographic featuresJaundice is a common indication for imaging. Often a specific cause will not be found, and the main role is differentiating between a non-obstructive and obstructive jaundice. In the latter (obstructive), extrahepatic and/or intrahepatic bile duct dilatation can be expected, depending on the level of obstruction. Hepatobiliary ultrasound and MRCP are the mainstay imaging modalities. Bilirubin levels are often too elevated for CT cholangiography to be performed. Treatment and prognosisManagement depends on the underlying etiology. In jaundiced neonates, phototherapy and exchange transfusion should be considered. Complications Quiz questions
عدل سابقا من قبل د.كمال سيد في الأحد مايو 12, 2024 8:15 am عدل 1 مرات | |
| | | | د.كمال سيد
Admin
عدد المساهمات : 2461
نقاط : 4249
السٌّمعَة : 9
الجنس :
علم بلدك :
تاريخ الميلاد : 03/04/1950
تاريخ التسجيل : 30/07/2012
العمر : 74
الموقع : السودان - سنار
العمل/الترفيه : طبيب عمومى وموجات صوتية
الساعة الان :
دعائي :
| | موضوع: Biliary colic الخميس مايو 09, 2024 7:53 pm | |
| What is biliary colic?Biliary colic is a steady or intermittent ache in the (URQ) upper abdomen, usually under the right side of the rib cage. It happens when something blocks the normal flow of bile from the gallbladder. Bile is a liquid that helps to digest fats. Under normal circumstances, bile is made in the liver and stored in the gallbladder. When you eat a meal, bile passes from the gallbladder through the cystic duct and the common bile duct into the small intestine, where it mixes with partially digested food. Gallstones are the most common reason for biliary colic. If a gallstone blocks either of these ducts, the normal flow of bile into the intestine is disrupted. The muscle cells in the bile duct contract vigorously to try to move the stone, causing the pain of biliary colic. A stricture of the bile duct or a tumor also can block bile flow and cause biliary colic. Symptoms of biliary colicA person with biliary colic usually complains of an ache or a feeling of pressure in the upper abdomen. This pain can be in the center of the upper abdomen just below the breastbone, or in the upper right part of the abdomen near the gallbladder and liver. In some people, the abdominal pain spreads back toward the right shoulder blade. Many people also have nausea and vomiting. Because symptoms of biliary colic usually are triggered by the digestive system's demand for bile, they are especially common after fatty meals. The symptoms also can occur when a person who has been fasting suddenly breaks the fast and eats a very large meal. Diagnosing biliary colicAfter you describe your symptoms, your doctor will perform a physical examination, paying particular attention to the upper right portion of your abdomen (the area of your liver and gallbladder). Ultrasound, the same painless procedure used to produce pictures of babies in the womb, can be used to produce pictures of your abdomen so your doctor can look for gallstones. Blood tests also may be done, especially if you have any fever or if your pain persists. Expected duration of biliary colicMost episodes of biliary colic pass after 1 to 5 hours. After the most intense pain passes, your abdomen may continue to ache mildly for about 24 hours. Preventing biliary colicBecause biliary colic is usually related to gallstones, it can be prevented by controlling the risk factors for gallstones. Some of these risk factors, such as heredity, increasing age and pregnancy, are a normal part of life. Others, such as obesity and a high-fat diet, are risk factors you can modify through a healthy lifestyle. Women going through menopause who take estrogen (h ormone replacement therapy) are also more likely to develop gallstones and biliary colic. Treating biliary colicAt first, your doctor may prescribe pain medication and encourage you to eat a fat-free diet. If the first episode of biliary colic is particularly severe, or episodes of colic keep retuning, surgery to remove the gallbladder ( cholecystectomy) usually is recommended. This procedure can be done through small incisions using an instrument called a laparoscope. The procedure usually requires only a brief stay in the hospital, and some people can leave the hospital the same day they have their operation. It is the most widely used treatment in people troubled by painful gallstones, because it is very effective and safe, with no complications in more than 90 percent of cases. If surgery cannot be done and symptoms of biliary colic are lasting, medication that dissolves gallstones may be used. However, this medication is expensive and can take months or years to work. Also, only small stones will dissolve. Rarely, medication to dissolve gallstones is combined with a procedure called shock-wave lithotripsy, which uses carefully aimed shock waves to break up gallstones. However, in many people treated with medication or lithotripsy, gallstones tend to form again within a few years. When to call a professionalCall your doctor whenever you have severe abdominal pain, with or without nausea and vomiting. If you have symptoms of biliary colic and you suddenly develop a fever and shaking chills, this may signal a gallbladder infection (cholecystitis), so call your doctor immediately. PrognosisAs long as you have gallstones that can block your cystic duct or common bile duct, you are at risk for repeated episodes of biliary colic. There is also a 25 percent chance that you will develop acute cholecystitis, or some other complication of gallstones, within 10 to 20 years. | |
| | | | | | GB & BILIARY US | |
|
| | صلاحيات هذا المنتدى: | لاتستطيع الرد على المواضيع في هذا المنتدى
| |
| |
| |
|







